The most common indication for cytologic examination of urine specimens is hematuria. Other indications include surveillance for recurrent urothelial carcinoma in patients with a history of urothelial carcinoma and for surveillance of patients at increased risk for urothelial carcinoma (genetic or exposure such as to aniline dyes or cyclophosphamide). Urine cytology is not used for screening asymptomatic patients.
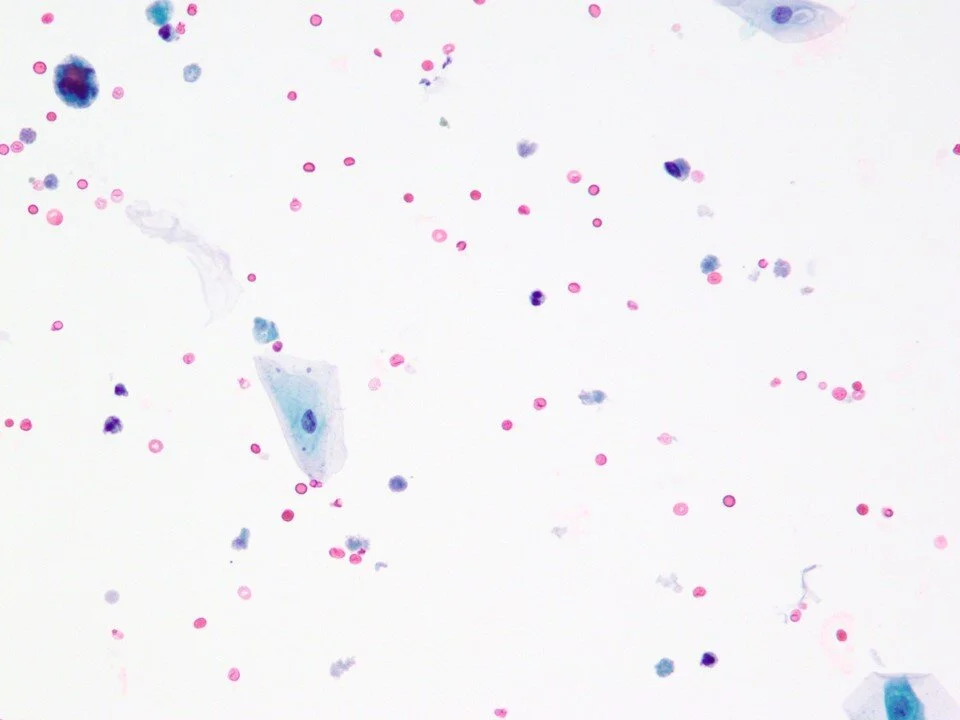
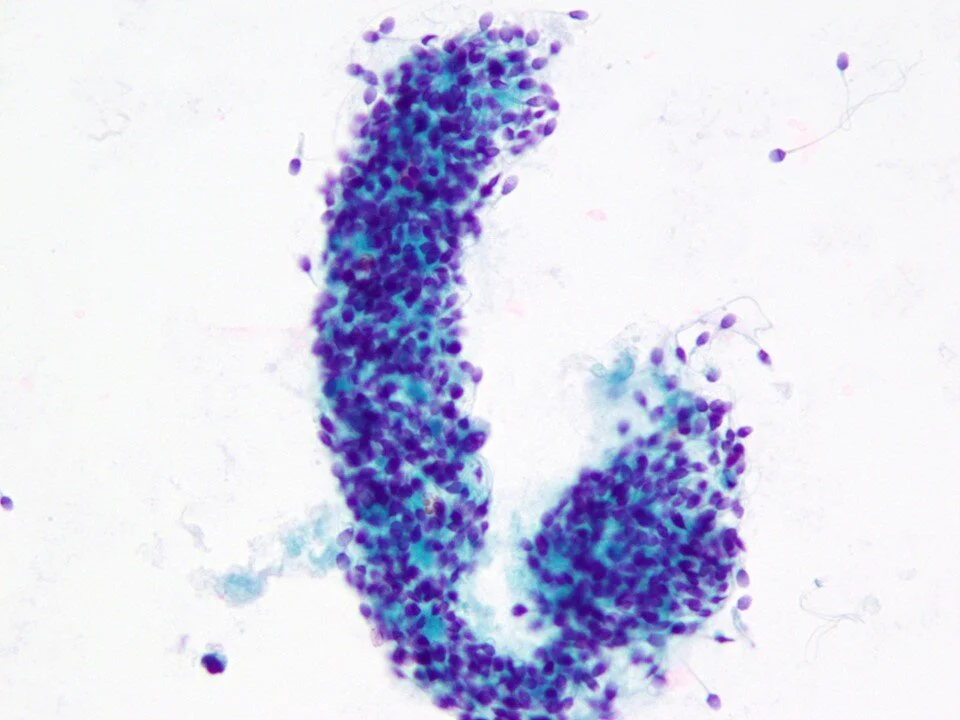
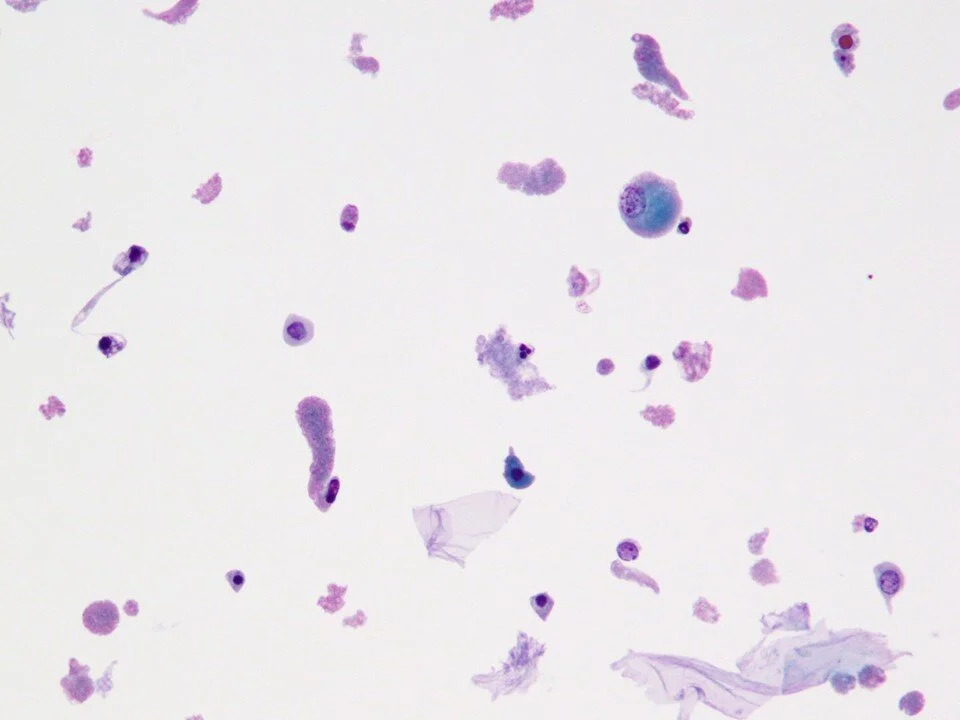
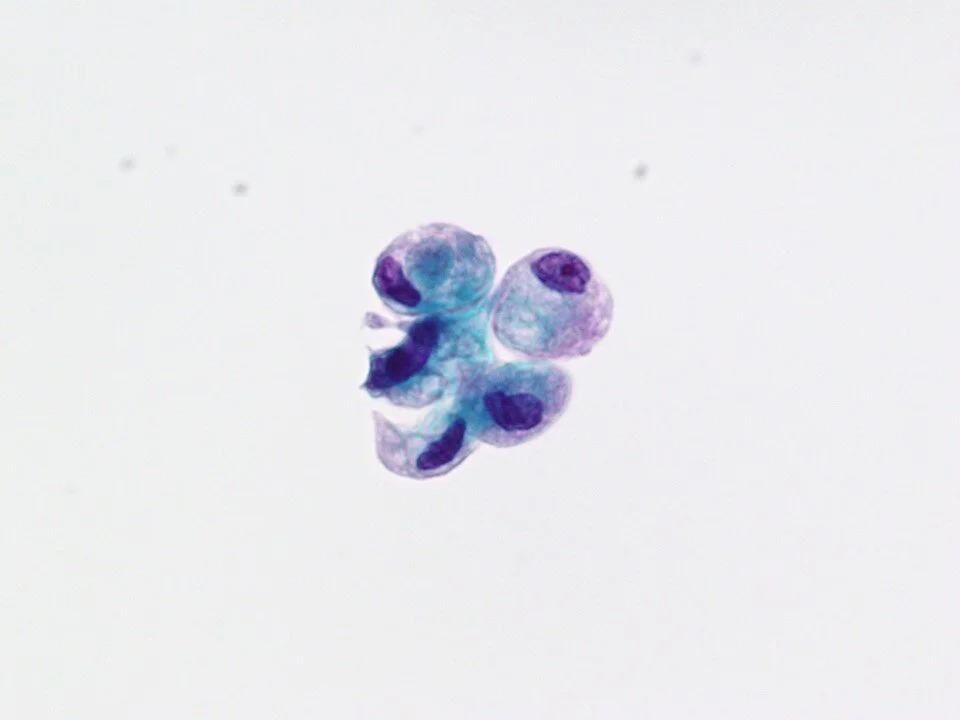
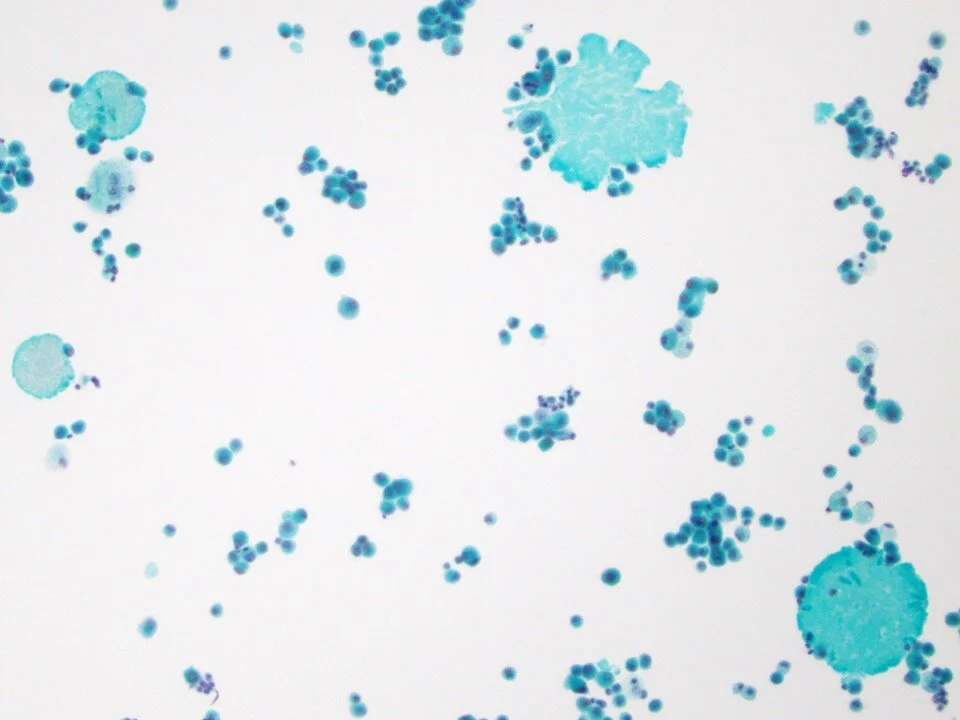
This sample was from a cystoscopy urine. Even without a noted history of instrumentation, some cytologic hints include the presence of urothelial cells in clusters as well as lubricant/gel material.
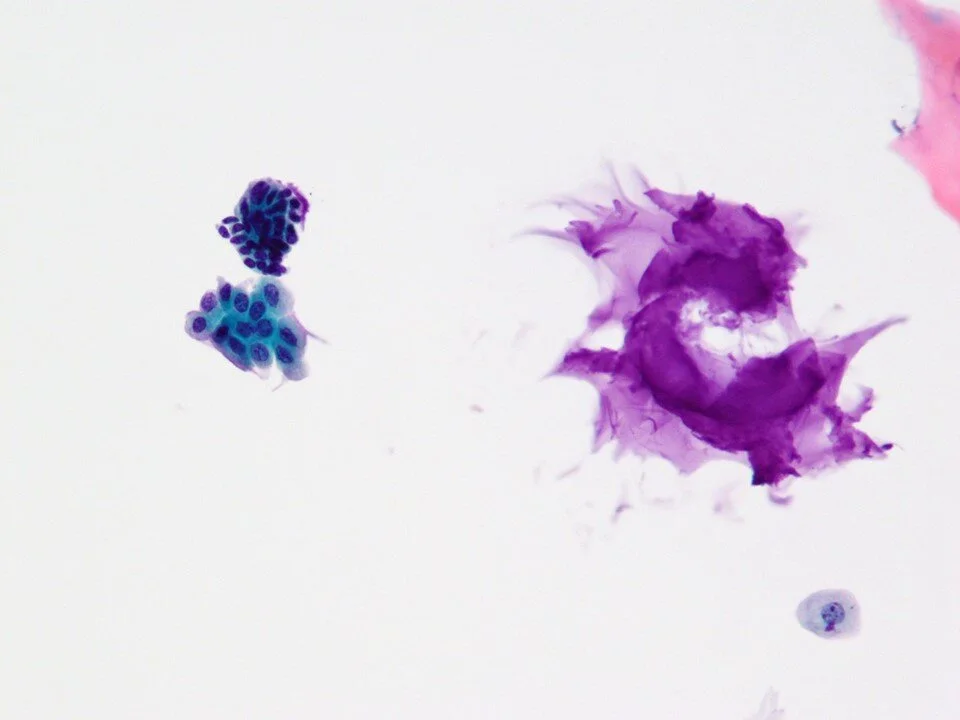
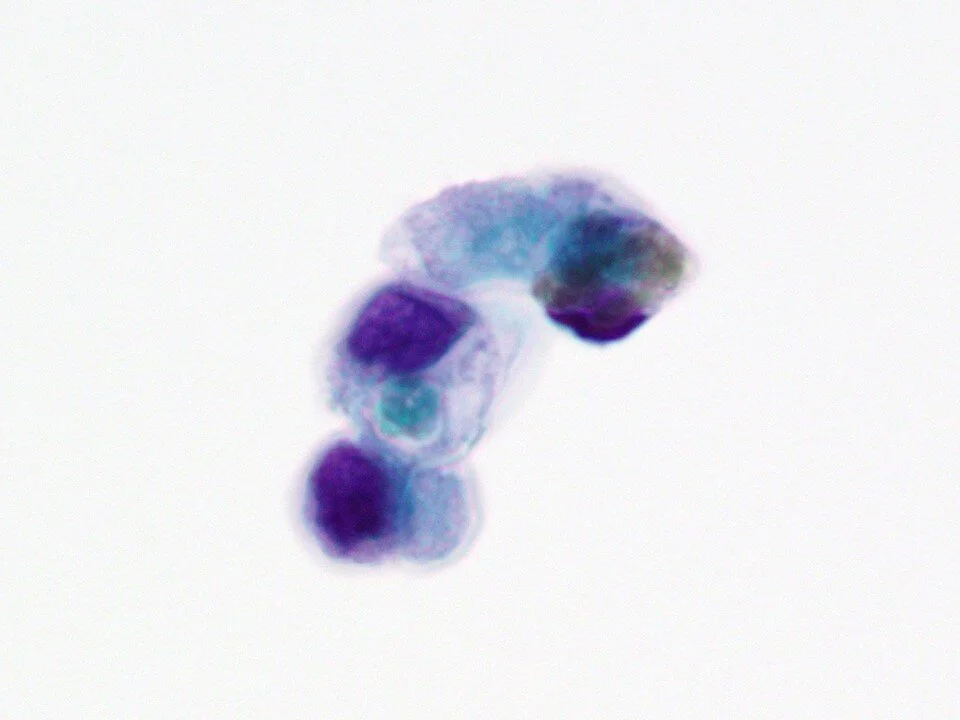
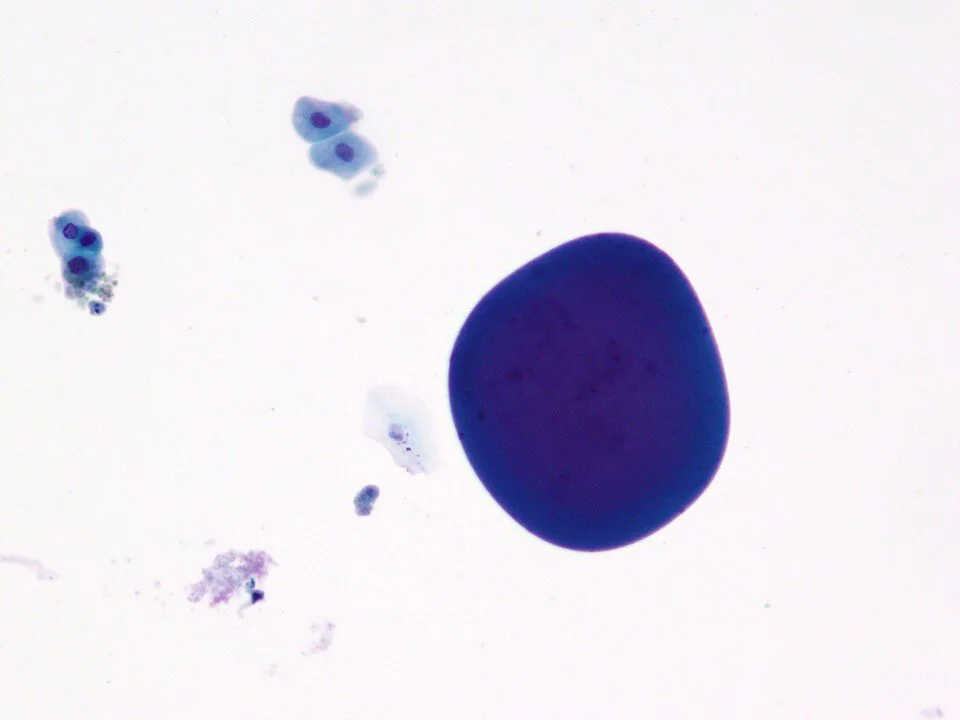
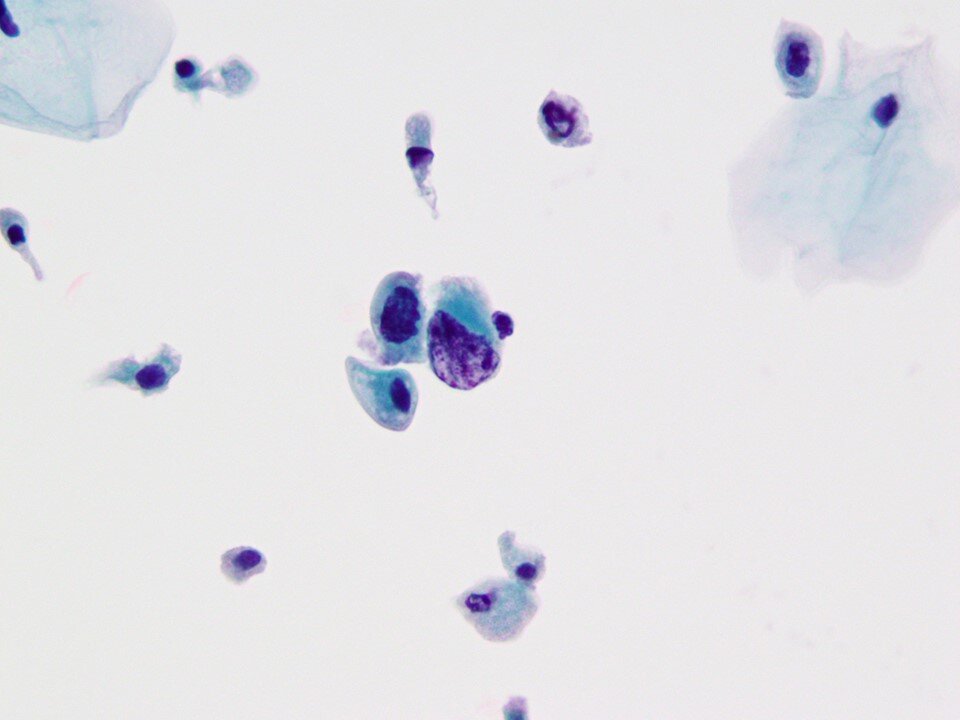
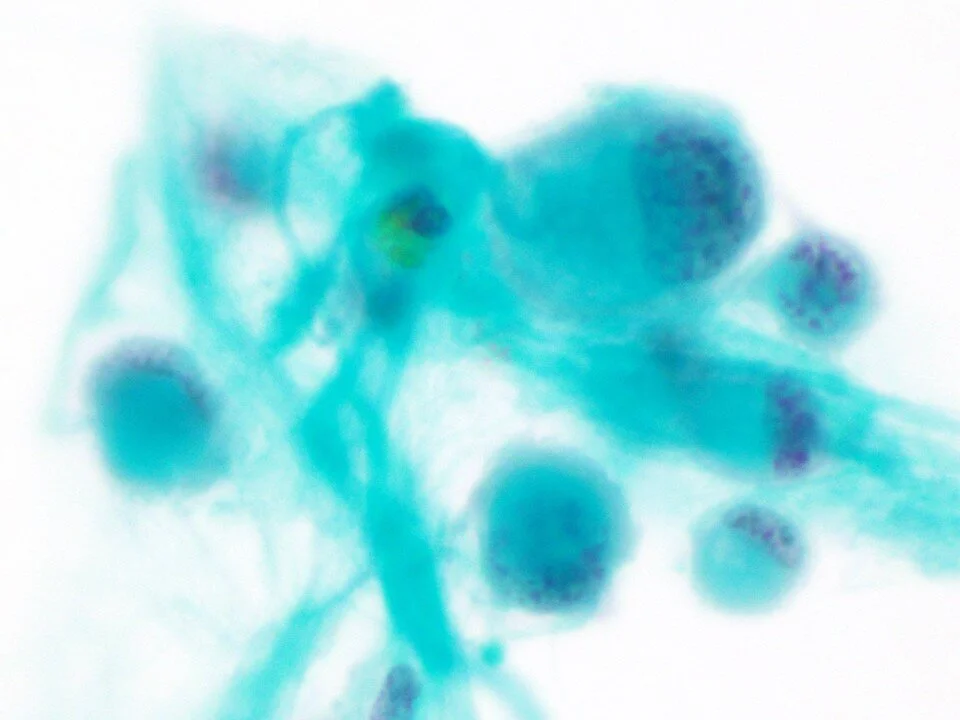
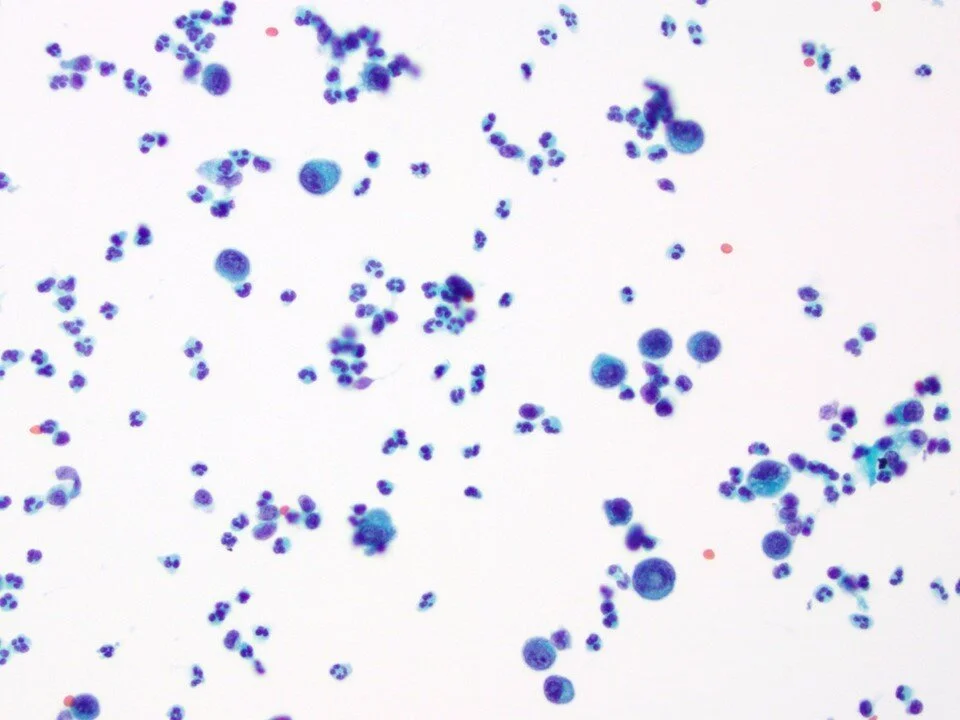
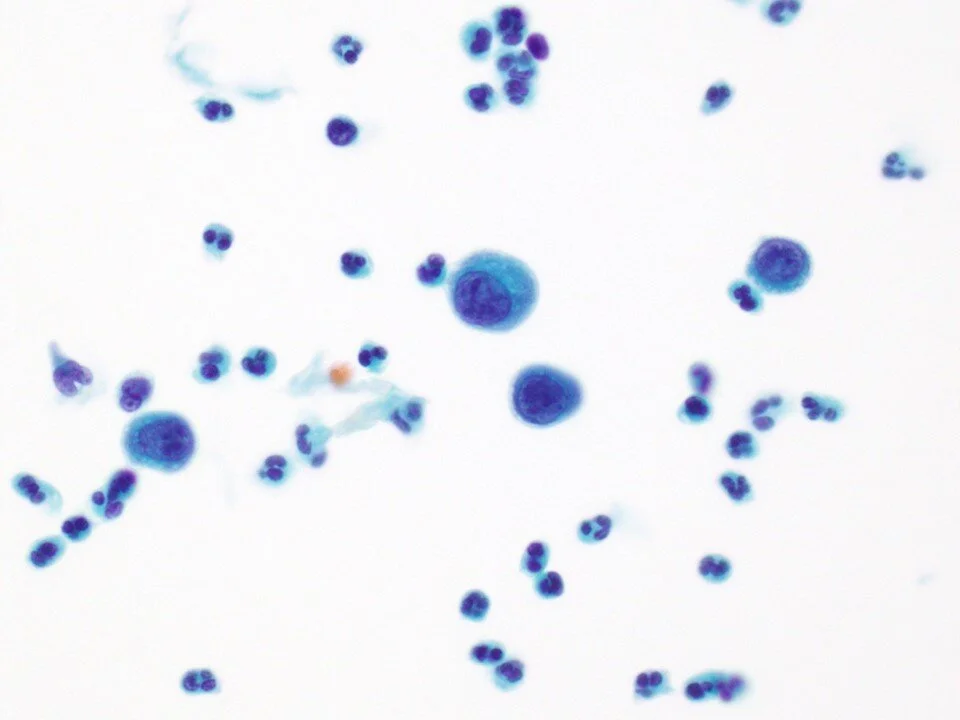
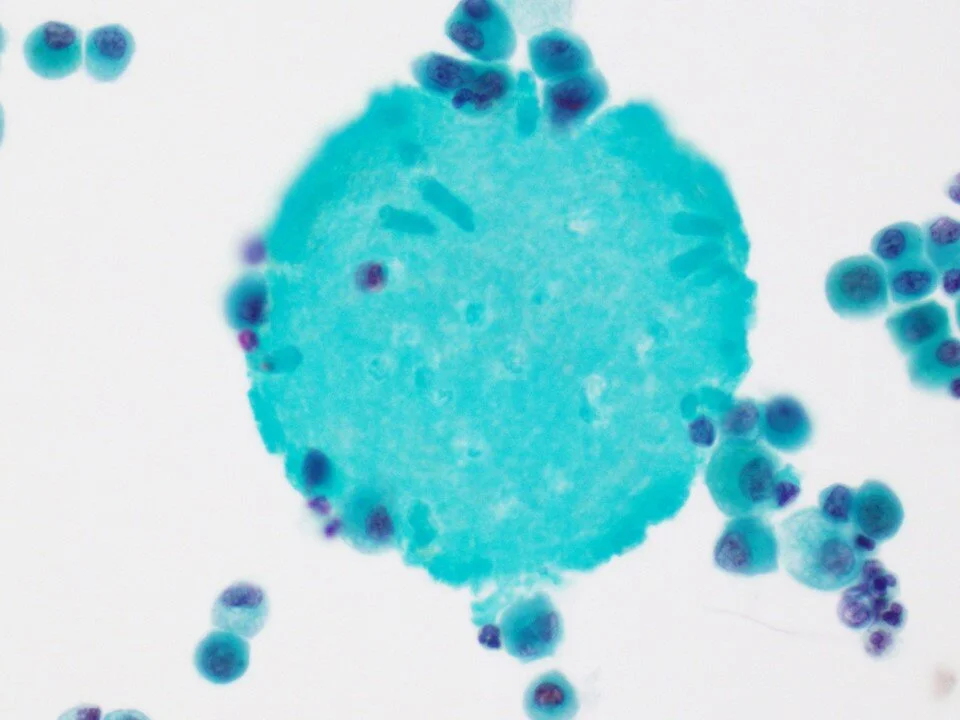
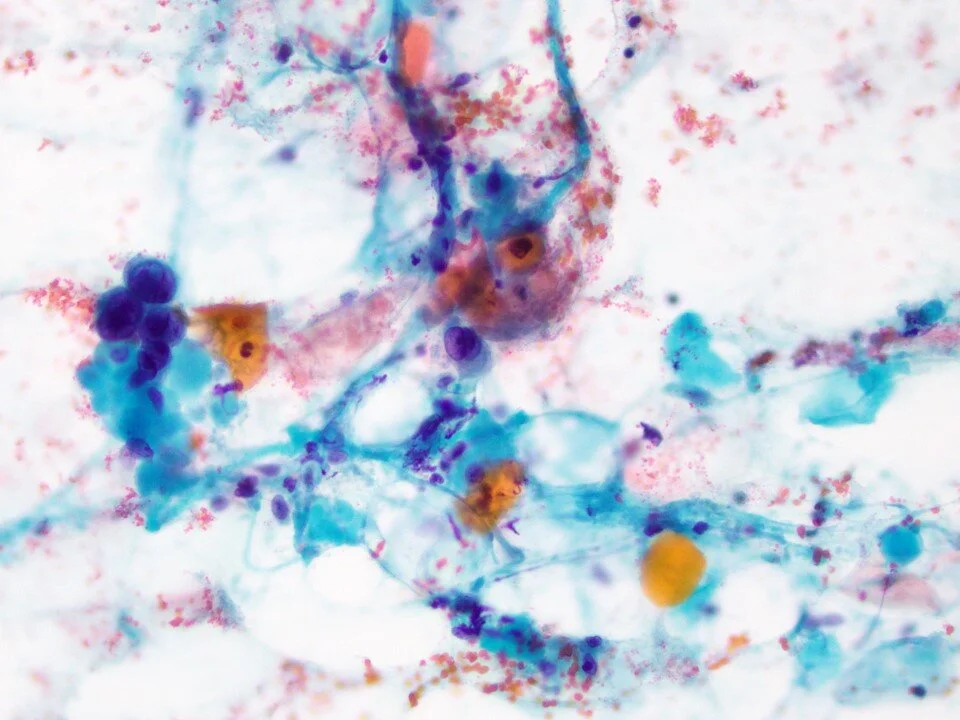
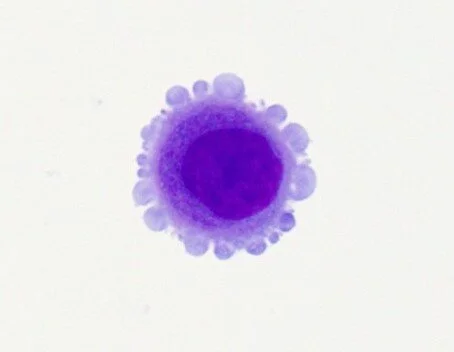
Superficial urothelial cells that cover the surface of the urothelium, referred to as umbrella cells. These are large cells that may be multinucleated.
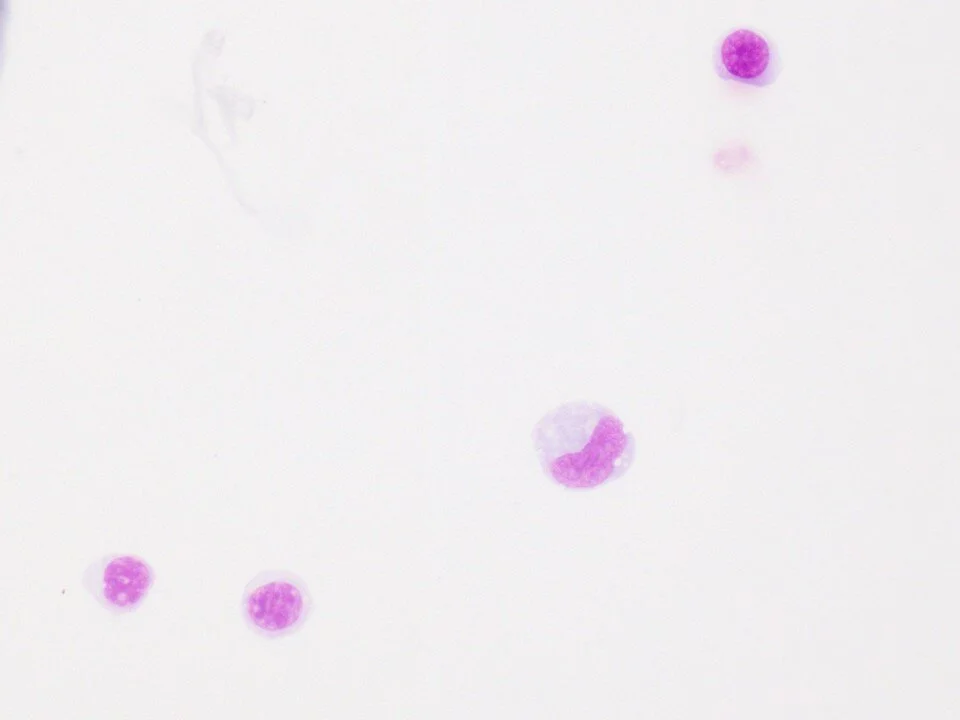
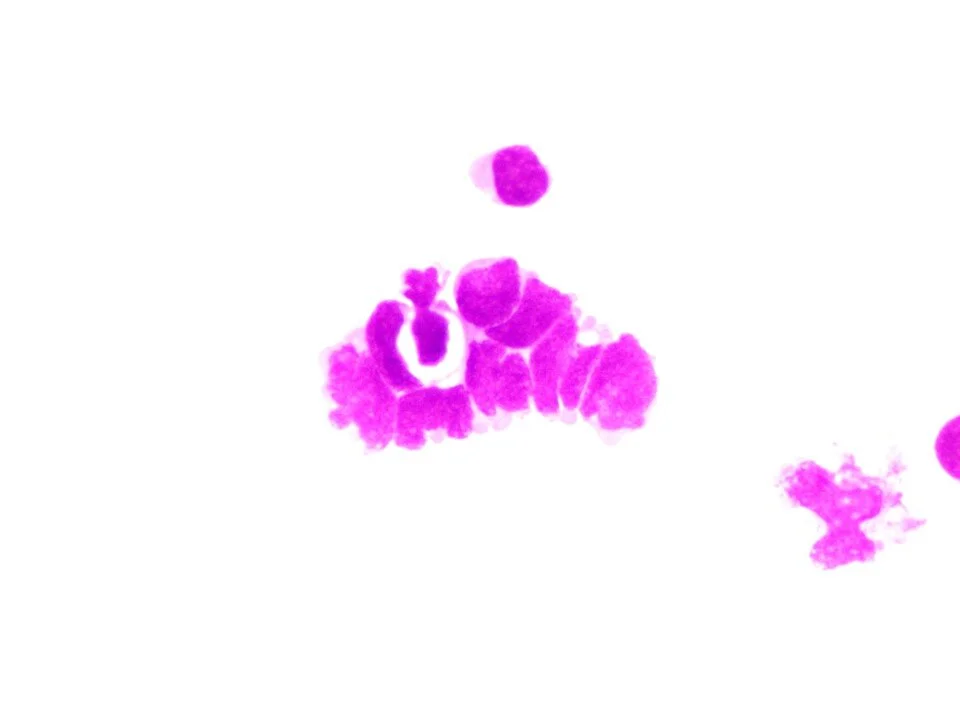
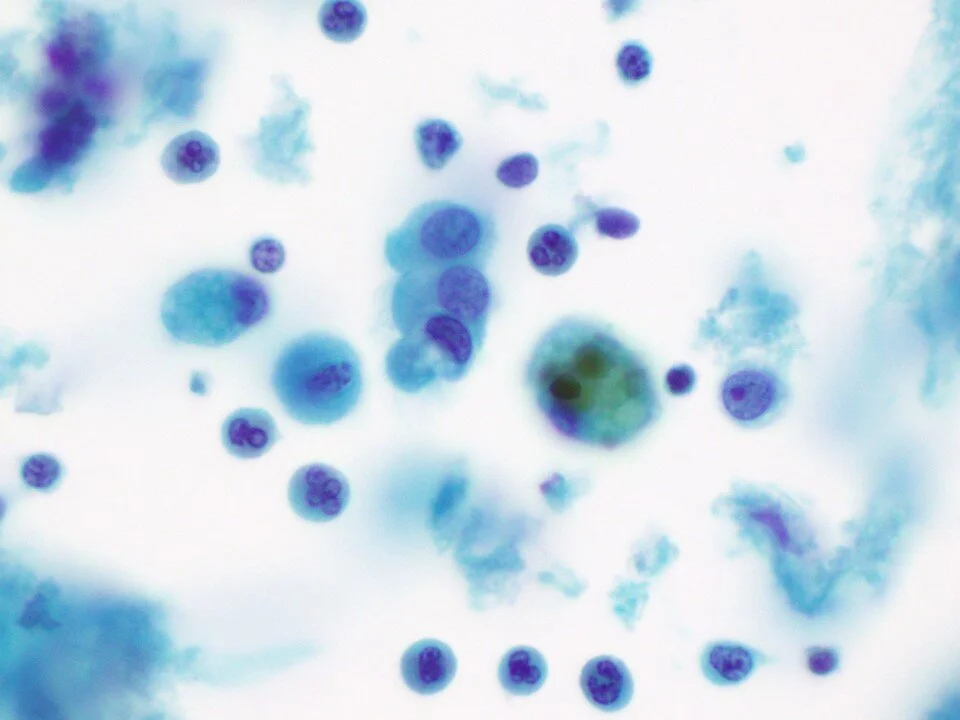
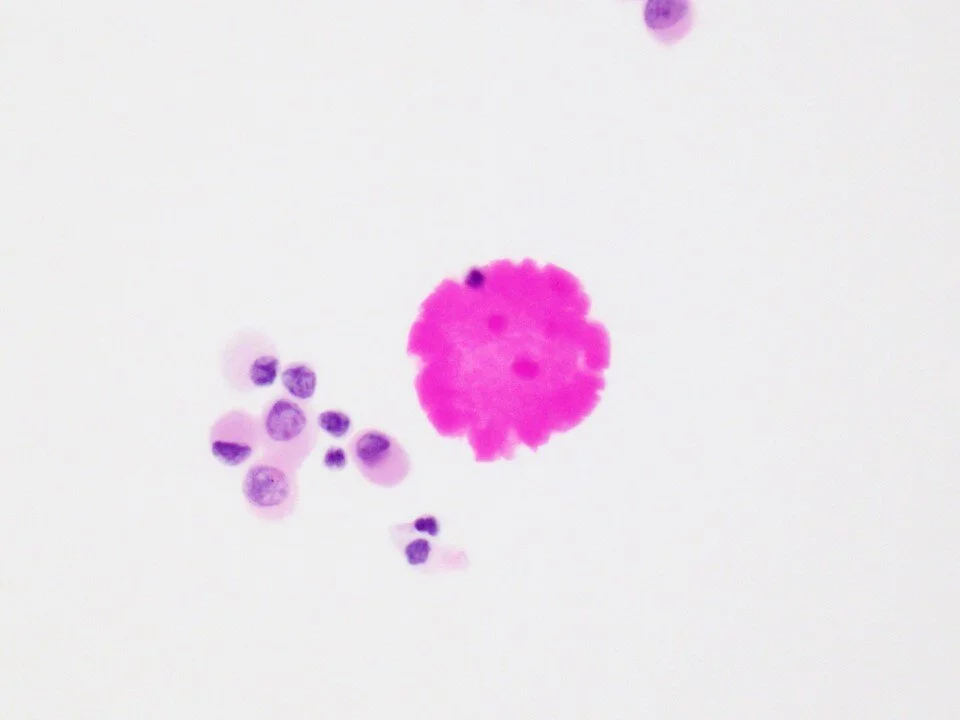
Degenerating urothelial cells may demonstrate characteristic “Melamed-Wolinska bodies” as seen here. These are pink-red (sometimes green) cytoplasmic inclusions. The exact pathogenesis of these bodies is not known. Their presence can be helpful when evaluating metastatic disease as they help indicate urothelial origin.
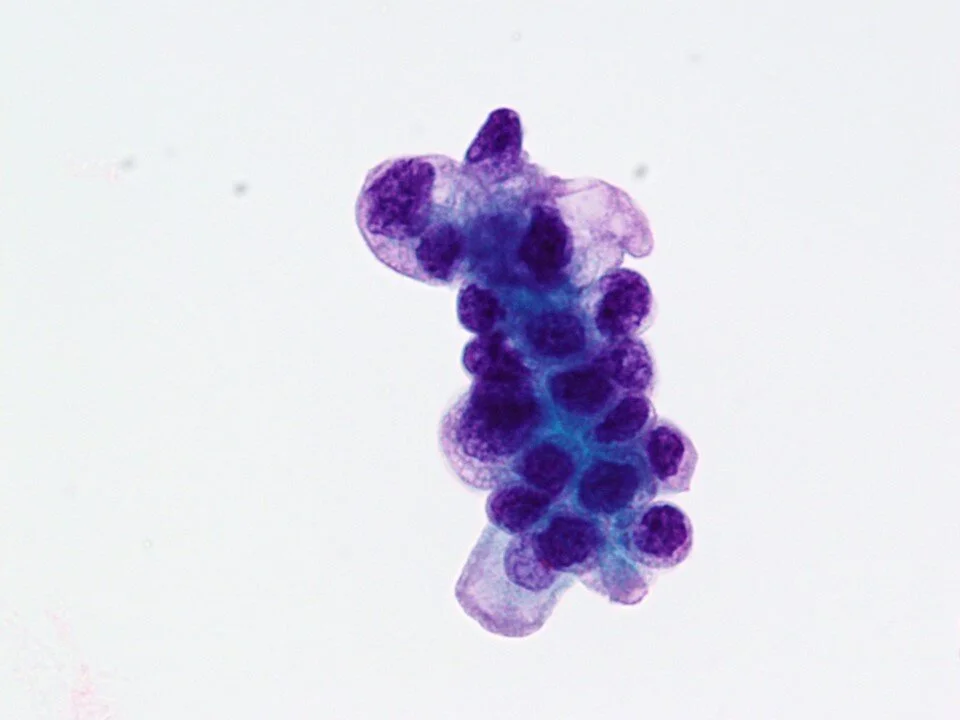
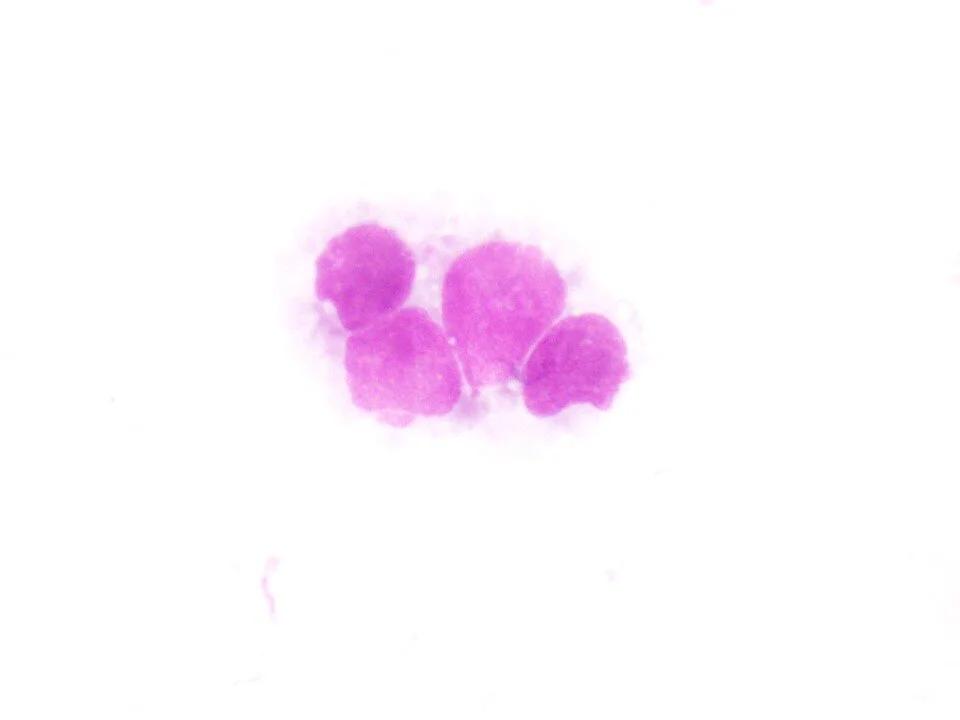
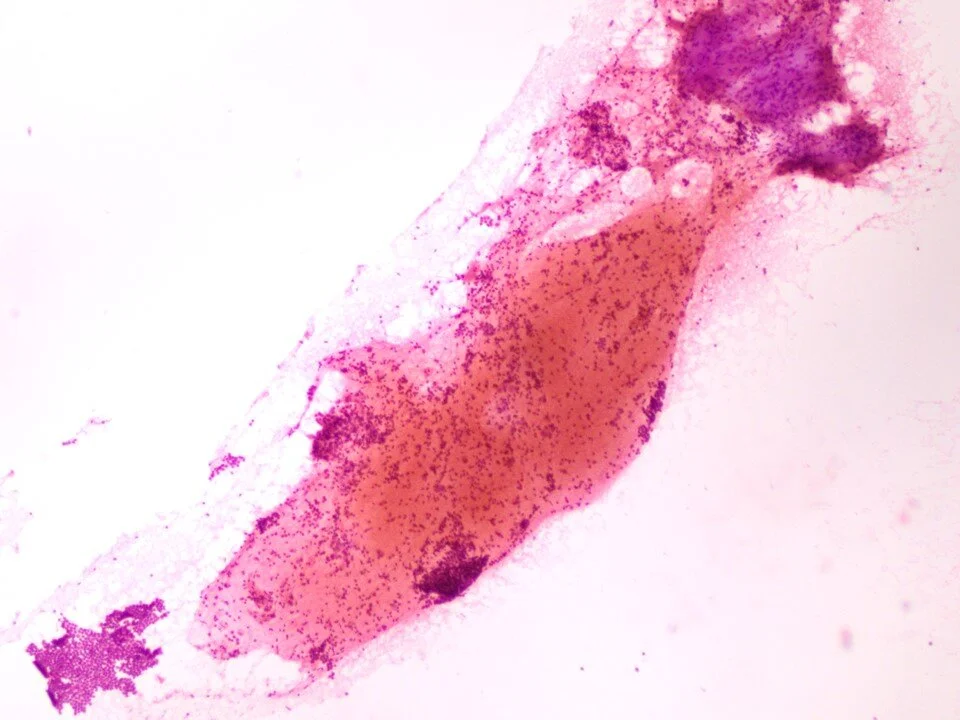
Sometimes large tissue fragments may be seen, even in voided specimens. This was a case from a patient with long history of cystitis glandularis.
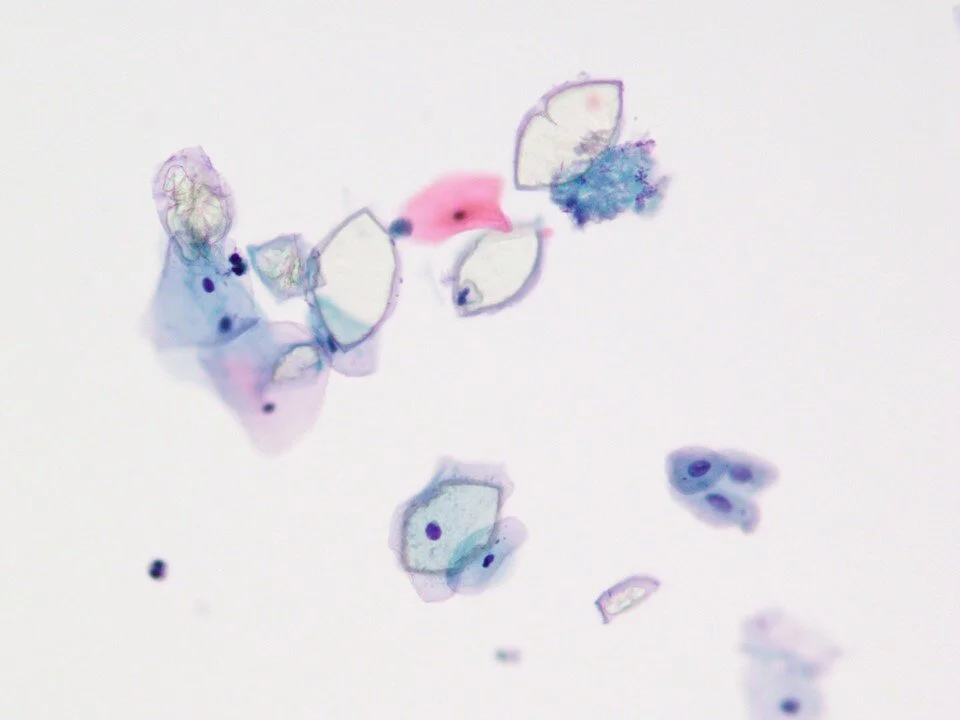
Glandular cells in the urine. Note the columnar shape.
Golden-brown cytoplasmic pigment (lipofuscin) helps identify these cells. Important to note as sometimes the nuclei tend to be hyperchromatic and should not be confused with atypical/malignant cells.
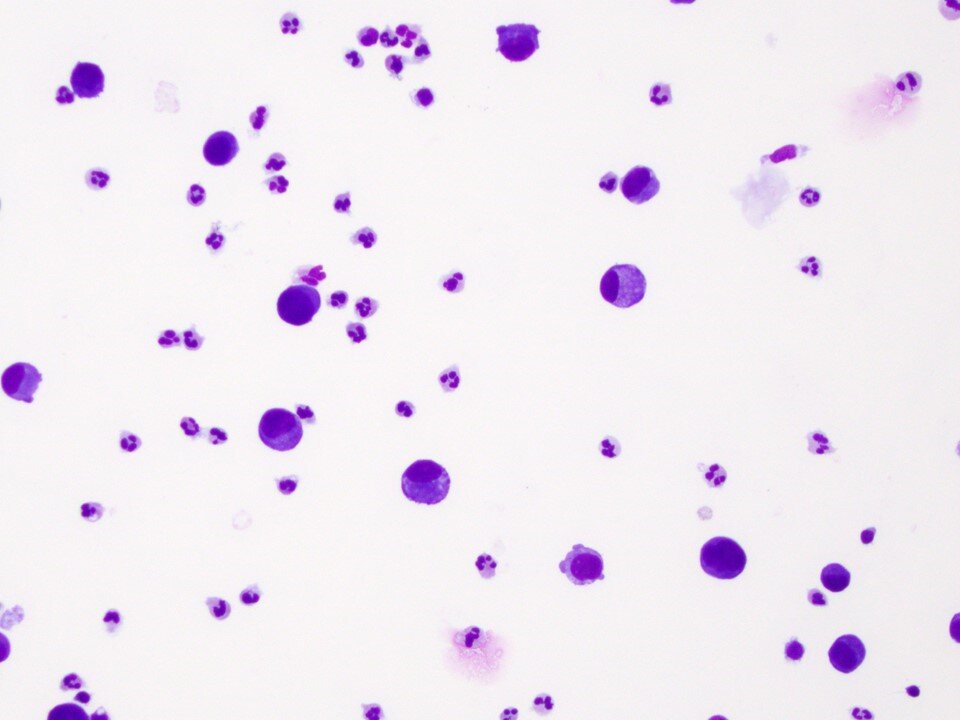
Most of the cells within ileal loop specimens are actually degenerated intestinal epithelial cells that may resemble macrophages.
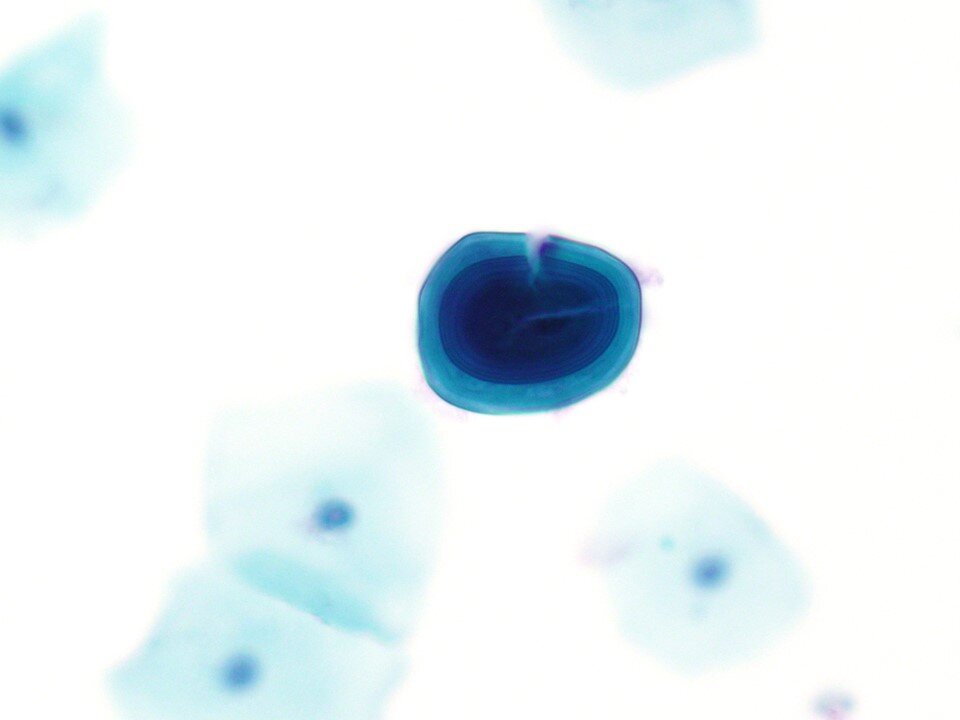
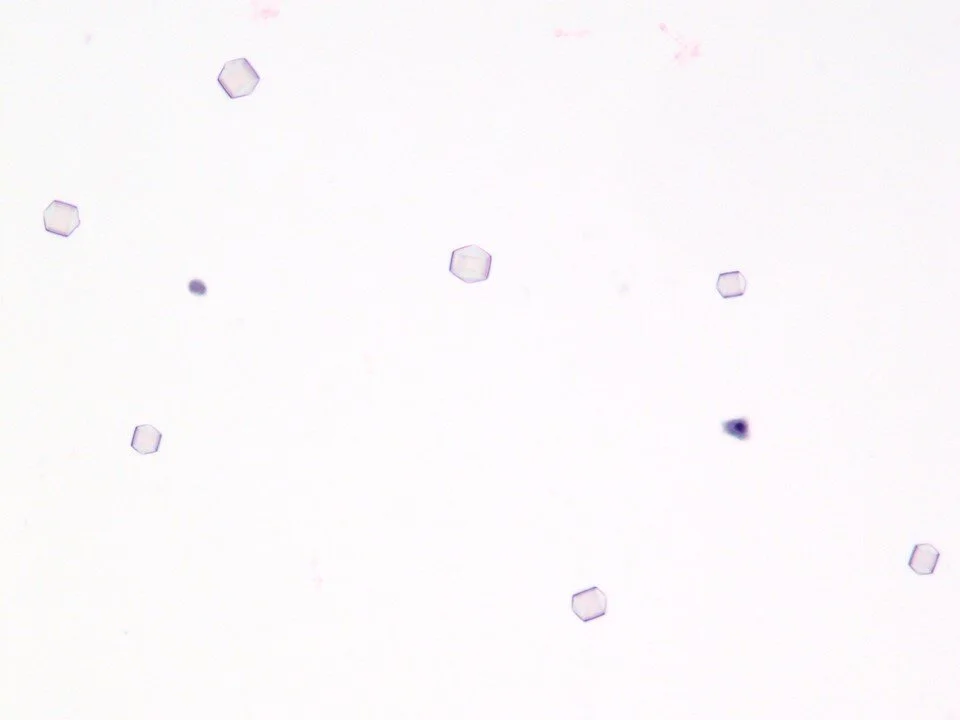
Crystals are a relatively common finding in urine samples.
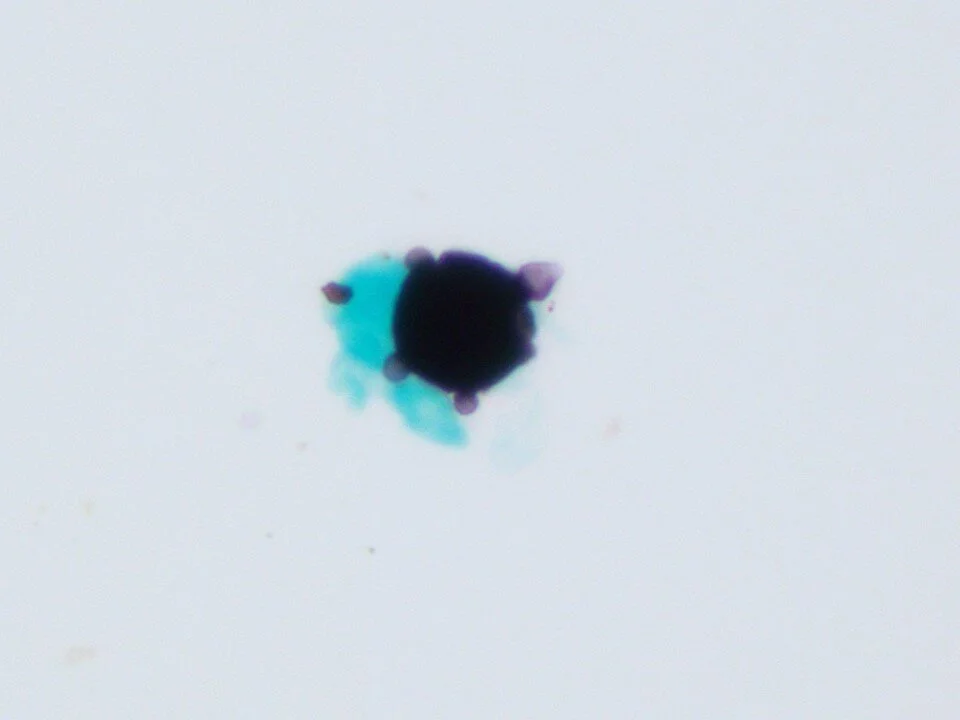
These should not be mistaken for crystals! Note the prominent “Maltese cross” seen in the center and in surrounding structures. This is a helpful hint that these are not crystals. Can be associated with applying powders, particularly those that are talc-based.
Casts can be seen in urine specimens, some with more clinical significance than others. A red blood cell cast is identified here.
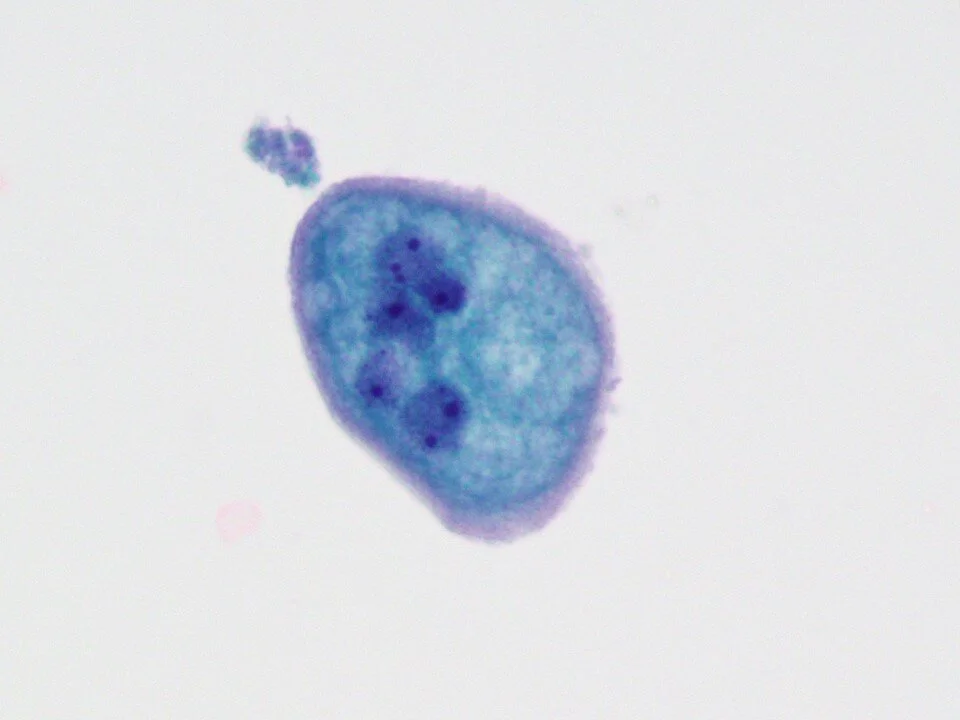
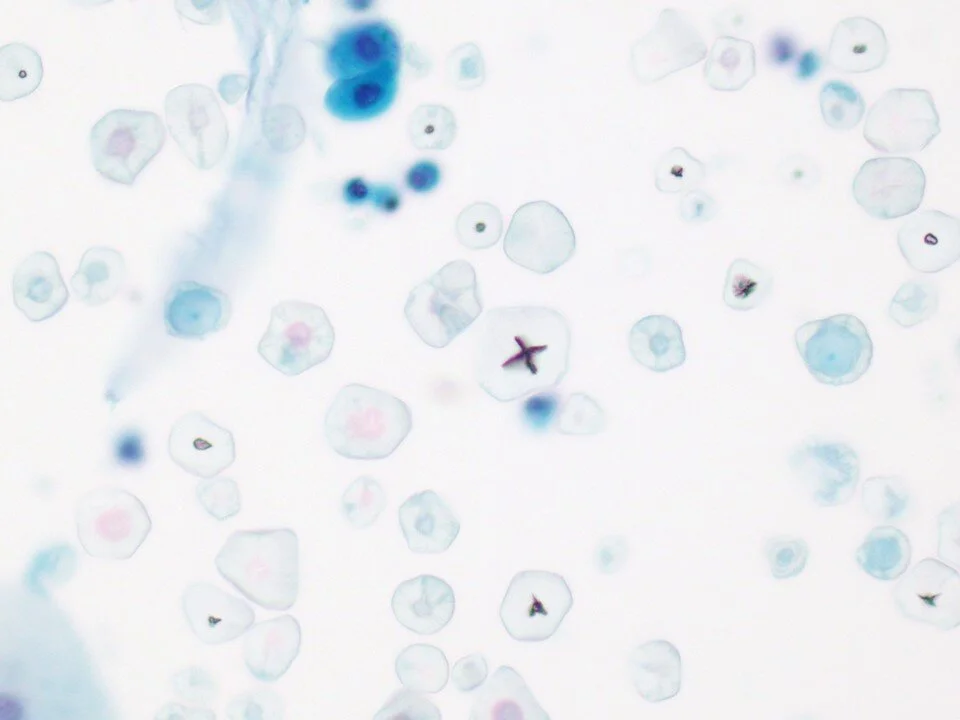
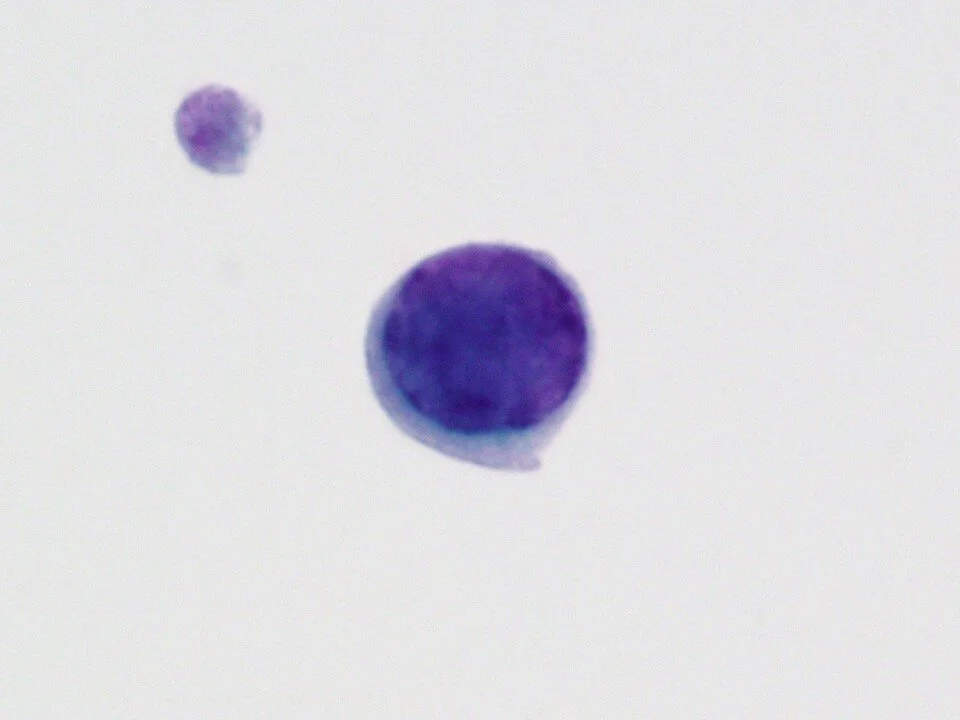
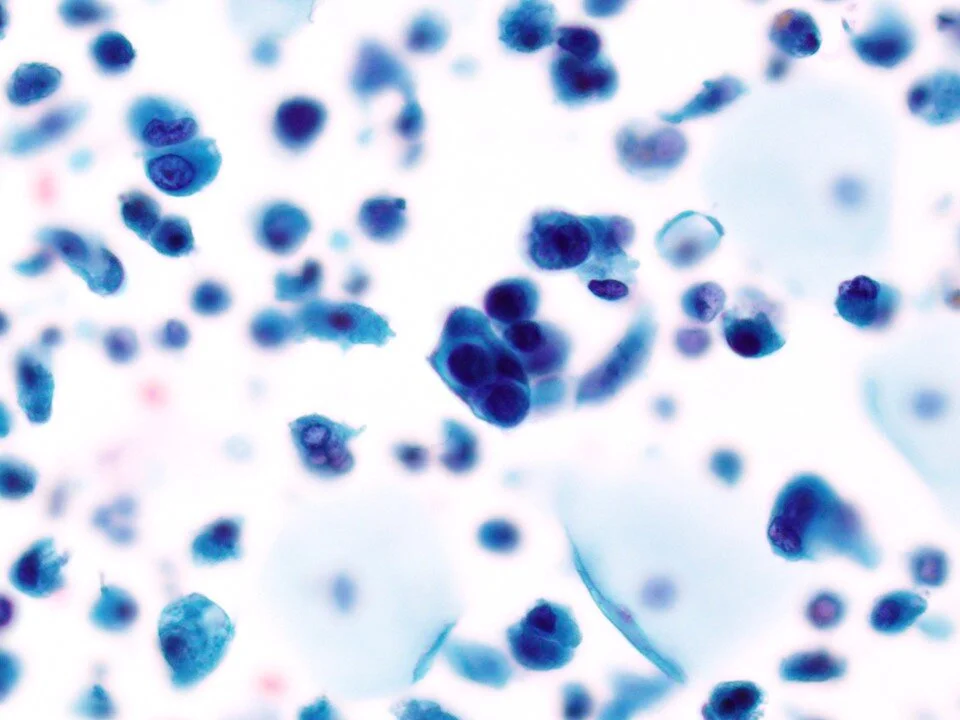
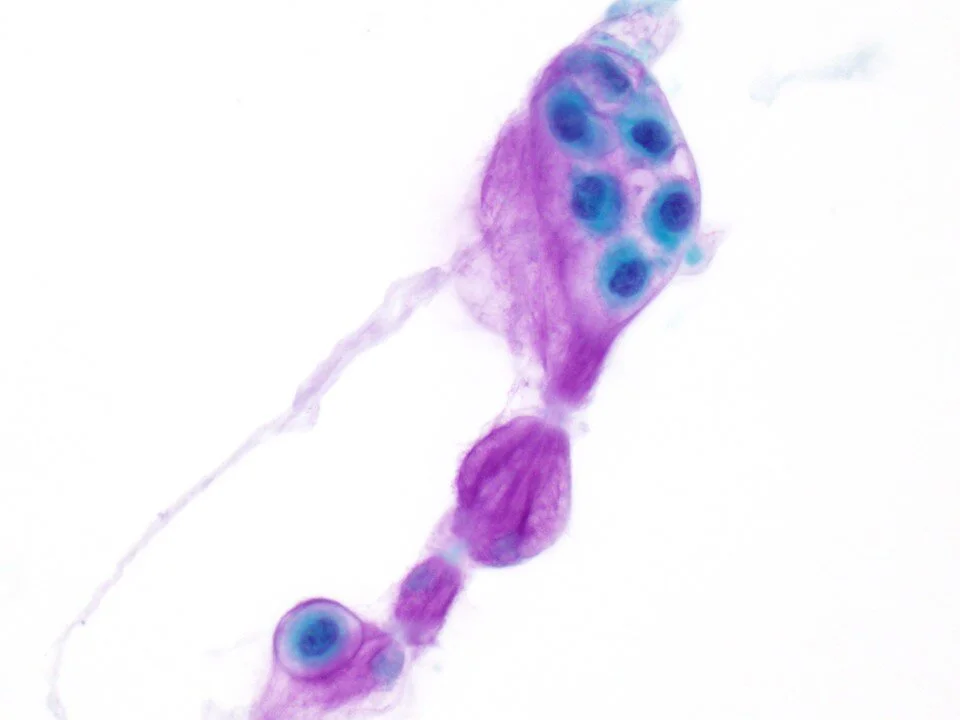
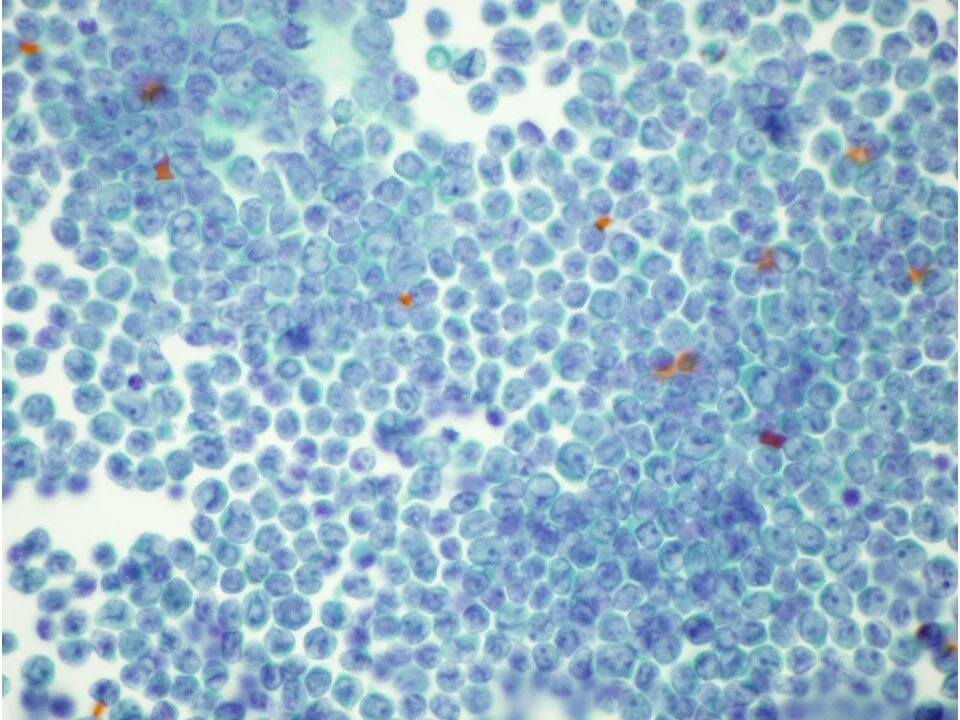
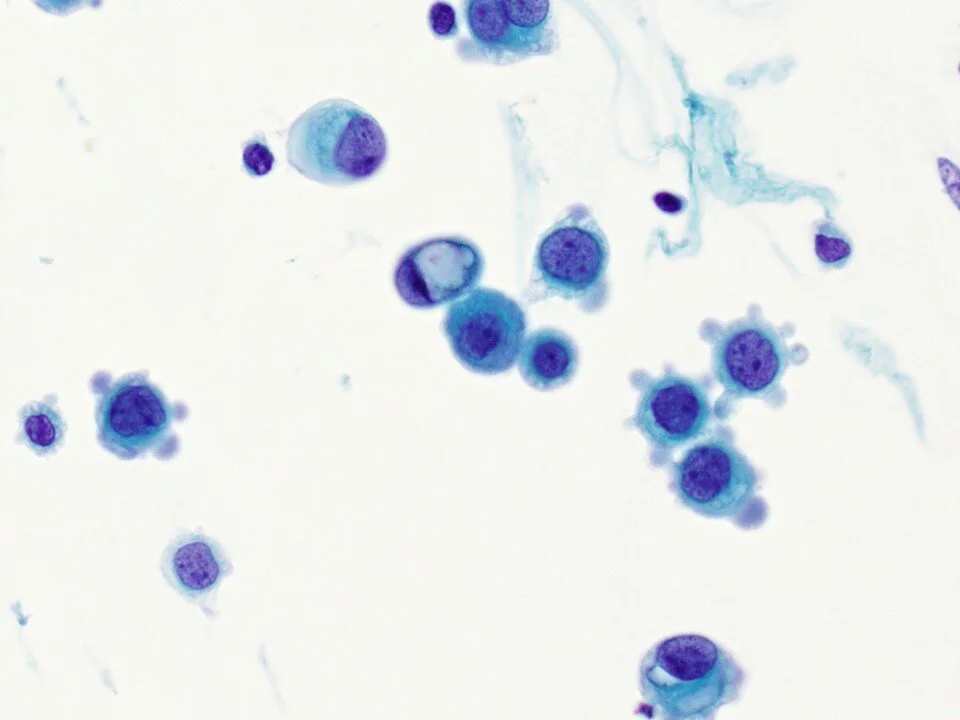
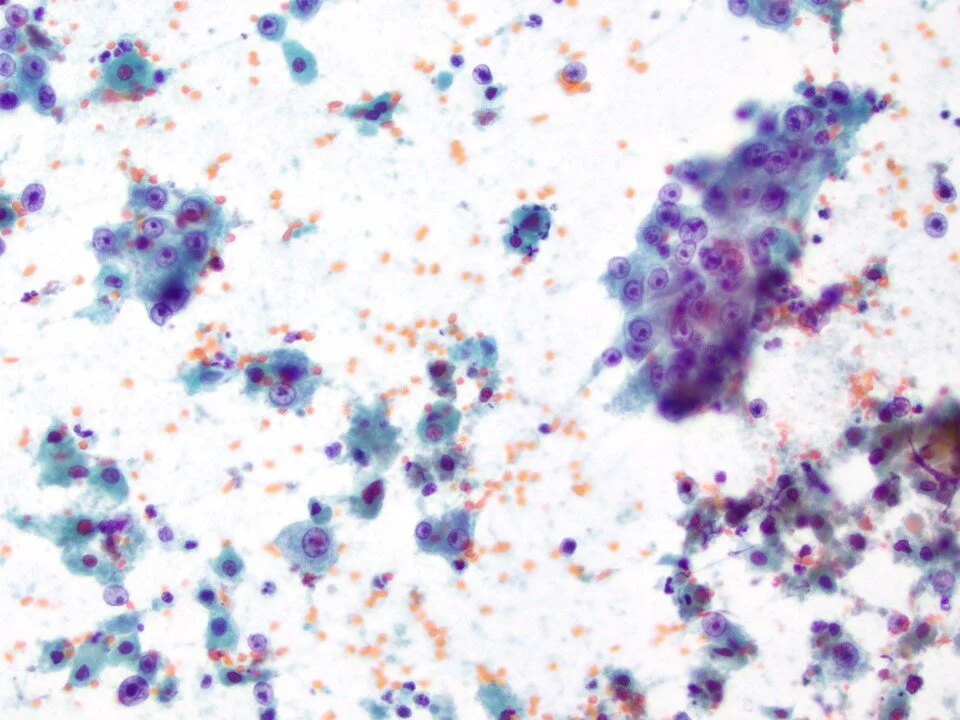
Sometimes referred to as “decoy cells,” PV cytopathic effect is important to recognize as the features may overlap with / mimic malignant cells. Although the nuclear to cytoplasmic (N:C) ratio is increased, note the very smooth nuclear borders and the glassy chromatin texture.
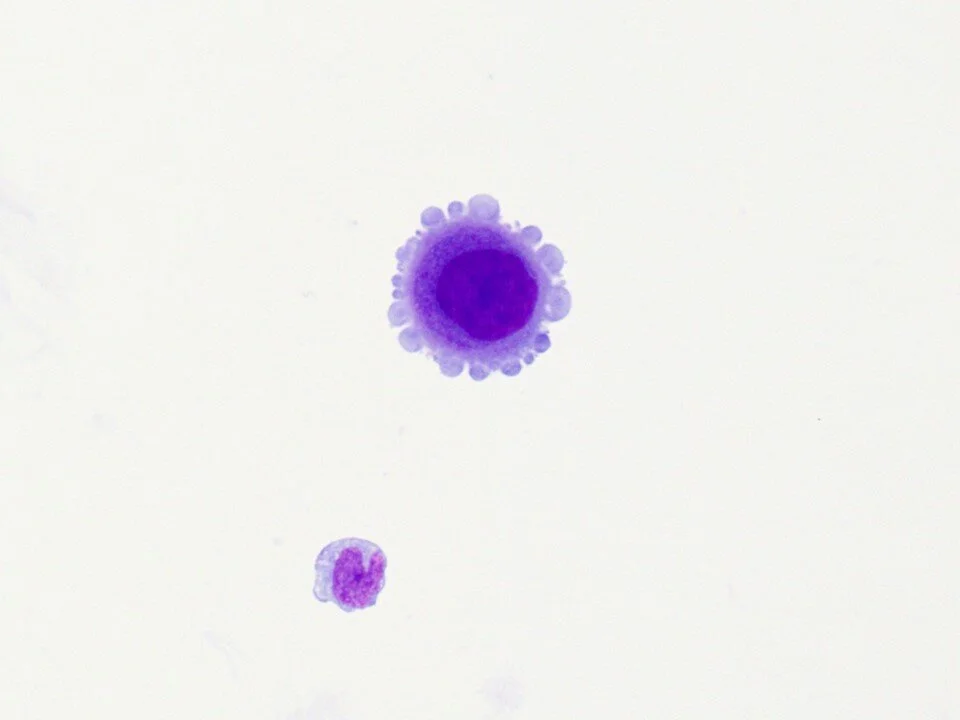
A granuloma (aggregate of histiocytes) is noted here. These can be seen with BCG therapy.
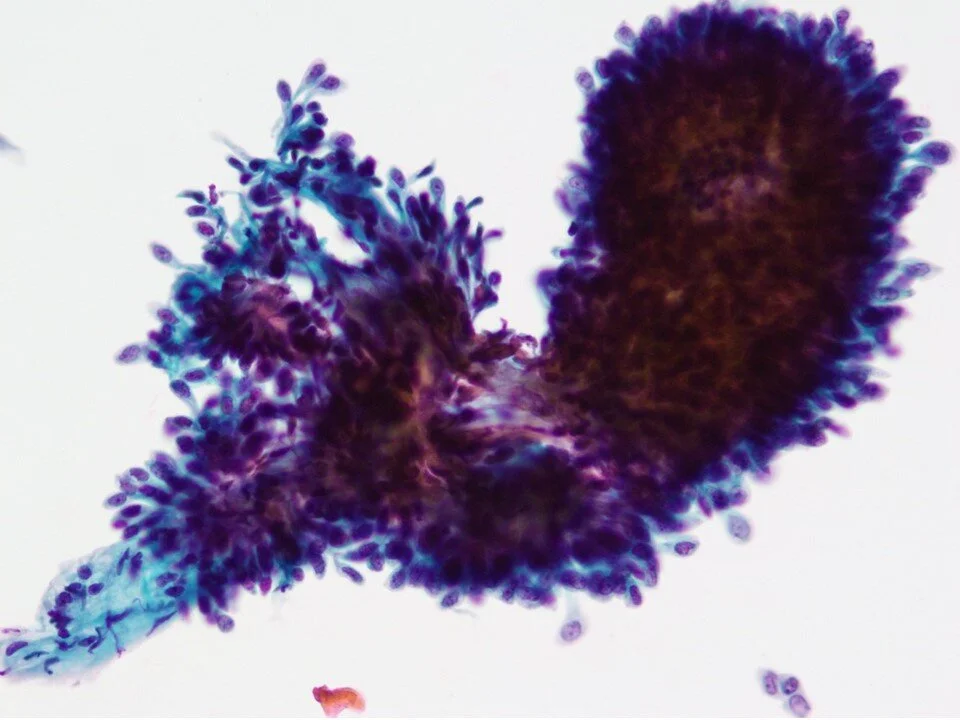
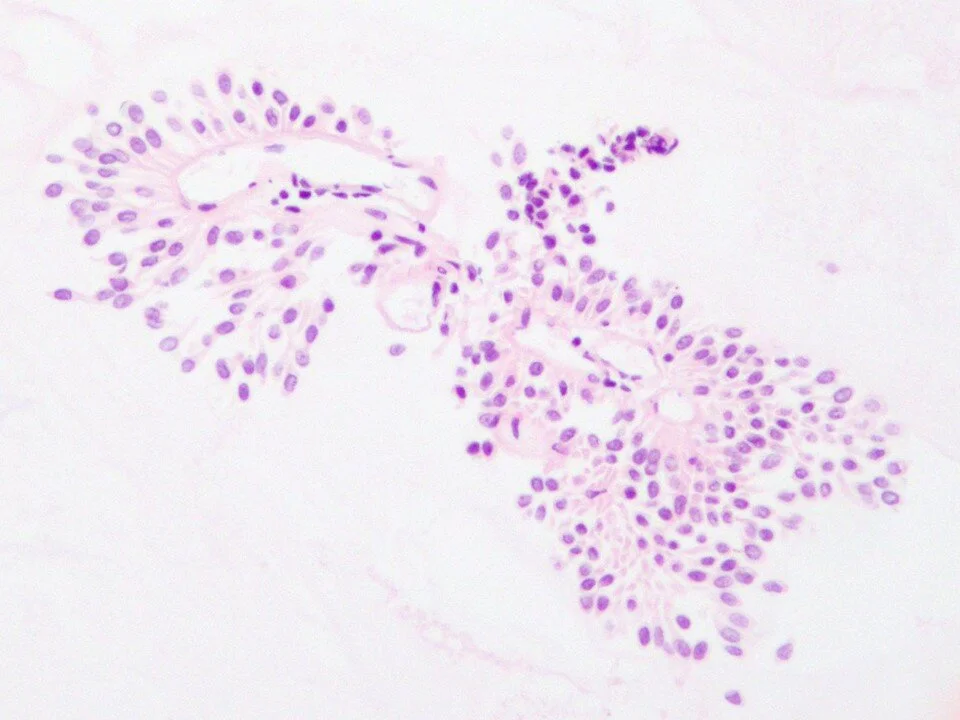
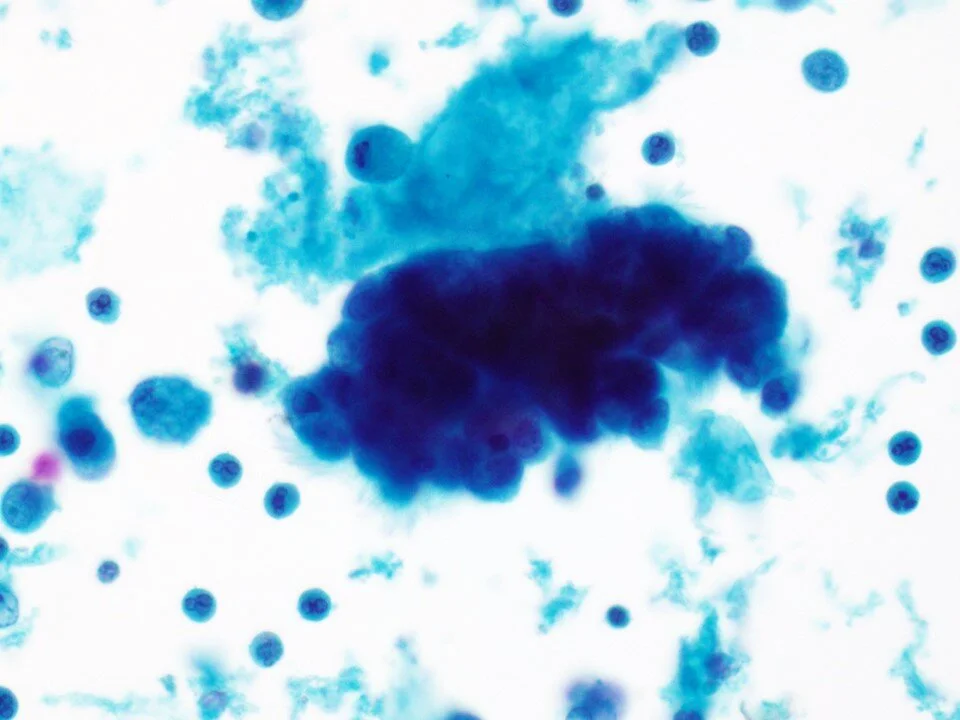
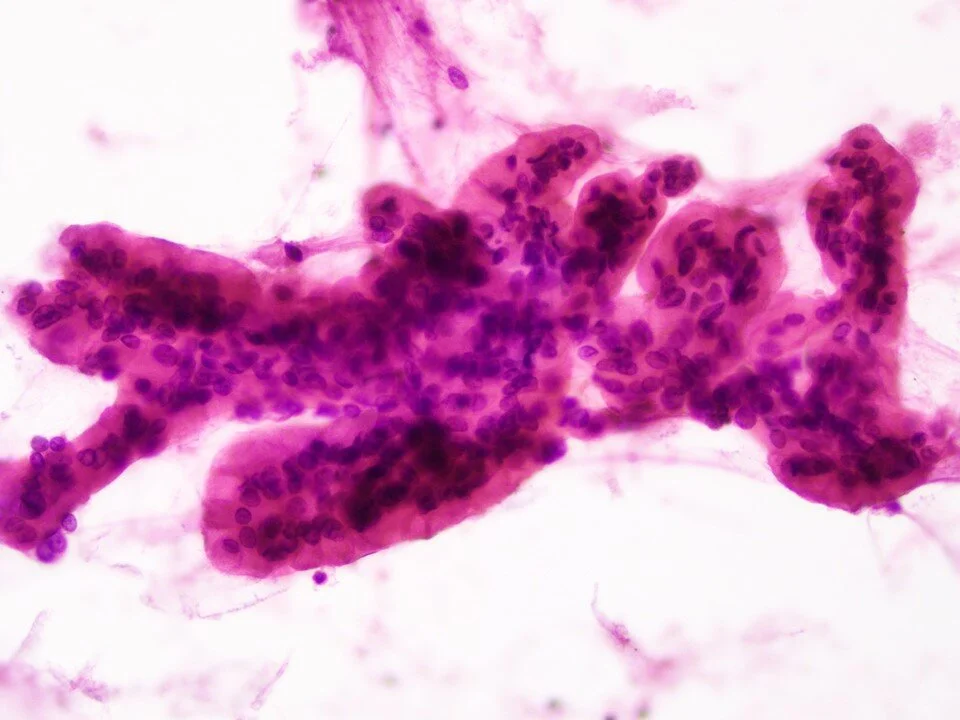
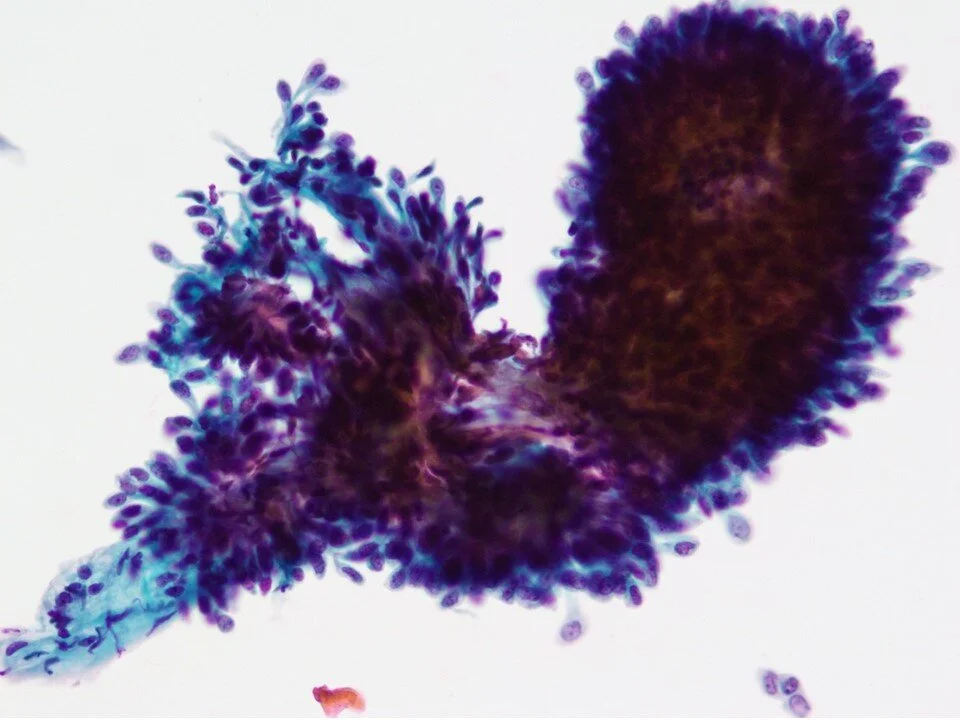
The main goal of the Paris System for Reporting Urinary Cytology is to identify High Grade Urothelial Neoplasia, largely in order to preserve the sensitivity and specificity of urine cytology due to the lack of reliability in diagnosing low grade lesions. However, there are features that can allow for the diagnosis of Low Grade Urothelial Neoplasm. Most importantly, the presence of fibrovascular cores (as seen here) is one such feature that can allow this diagnosis with the most degree of confidence.
Again, note the fibrovascular core seen here.
For reference, see The Paris System https://pubmed.ncbi.nlm.nih.gov/31042521/
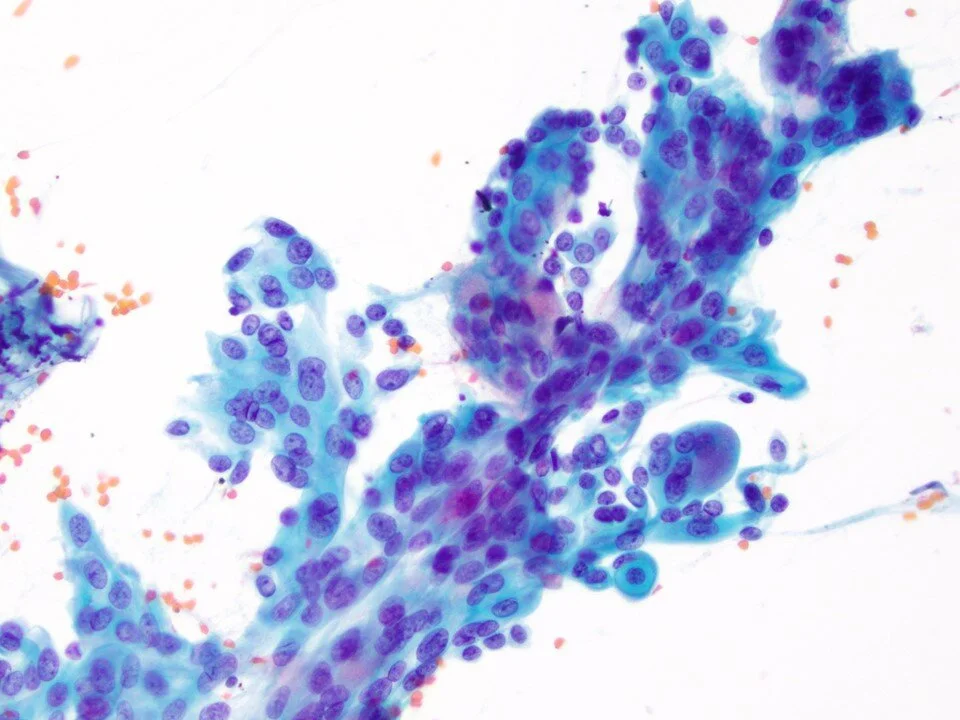
This cell block preparation highlights the fibrovascular core. In practice, cell blocks can be helpful to this end when in doubt as to the presence of fibrovascular cores within dense clusters of cells.
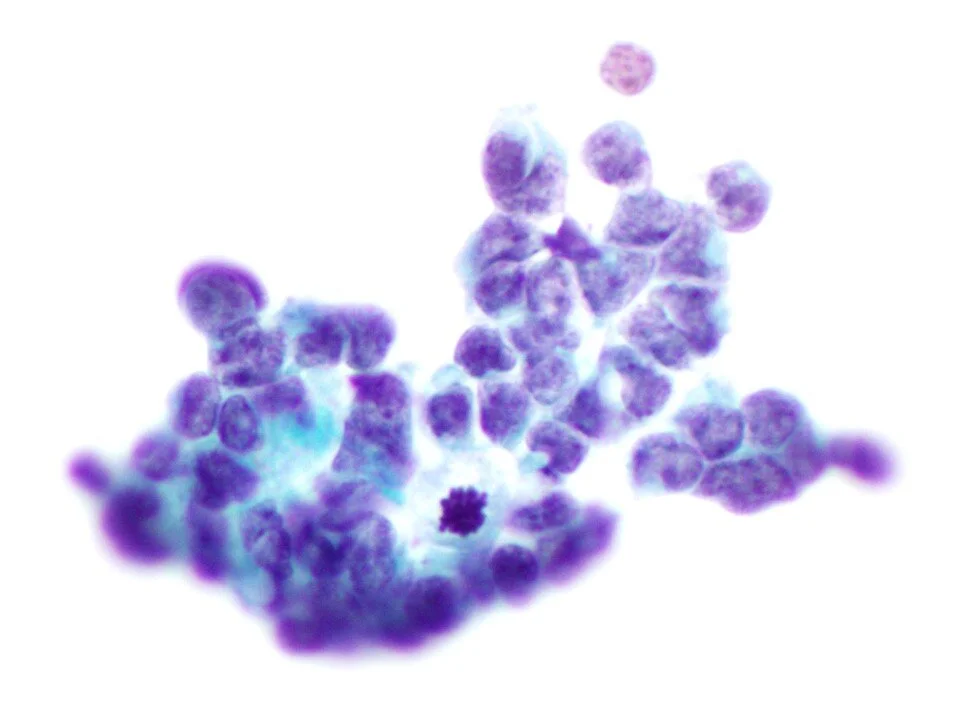
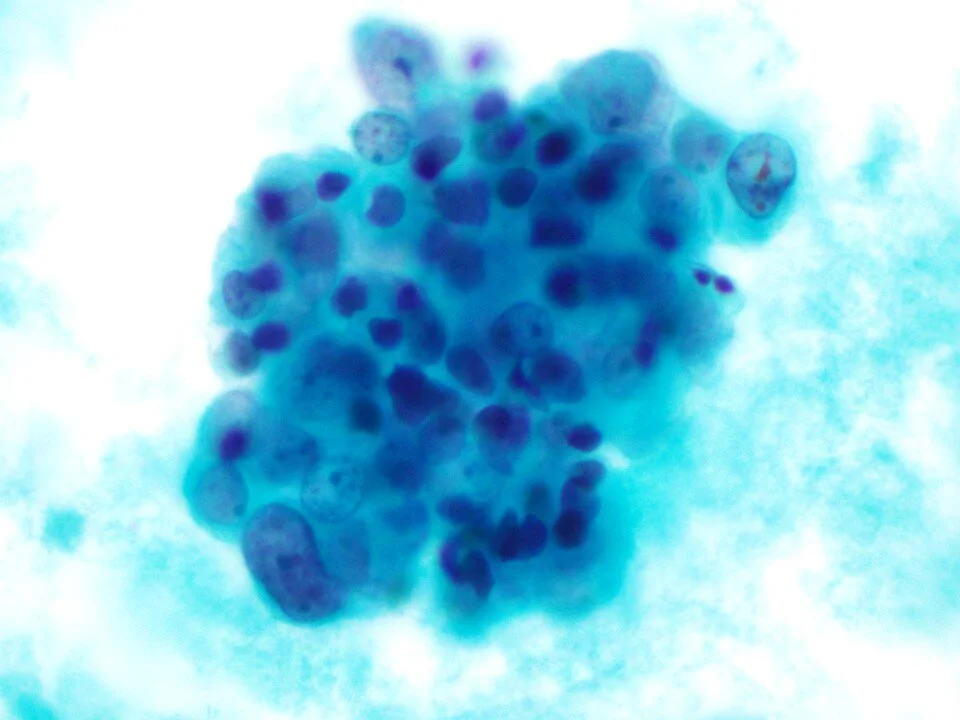
The Paris System highlights several criteria for the diagnosis of High Grade Urothelial Carcinoma. Cases are categorized (negative for high-grade urothelial carcinoma, atypical, suspicious for high-grade urothelial carcinoma, positive for high-grade urothelial carcinoma) based on these criteria.
Criteria for HGUC include examination of the N:C ratio (>0.7 for suspicious or positive), nuclear chromasia (hyperchromasia / very dark), nuclear membrane (uneven shape and thickness), and chromatin quality (coarsely clumped). The first two of these are considered “major” criteria. Other features include nuclear and cytoplasmic pleomorphism, eccentrically located nuclei, dense cytoplasm, pesence of mitotic figures, and apoptotic bodies.
Sometimes “entosis” may be seen, which is a form of cell cannibalism where a tumor cell appears to tightly wrap around another. Has a “bird’s eye” appearance.
Higher magnification to highlight malignant features including increased N:C ratio, hyperchromasia, and angulation of the nuclei
Metanephric adenoma is a challenging pitfall of urine cytology. The cytologic features can overlap with both benign/reactive as well as malignant processes.
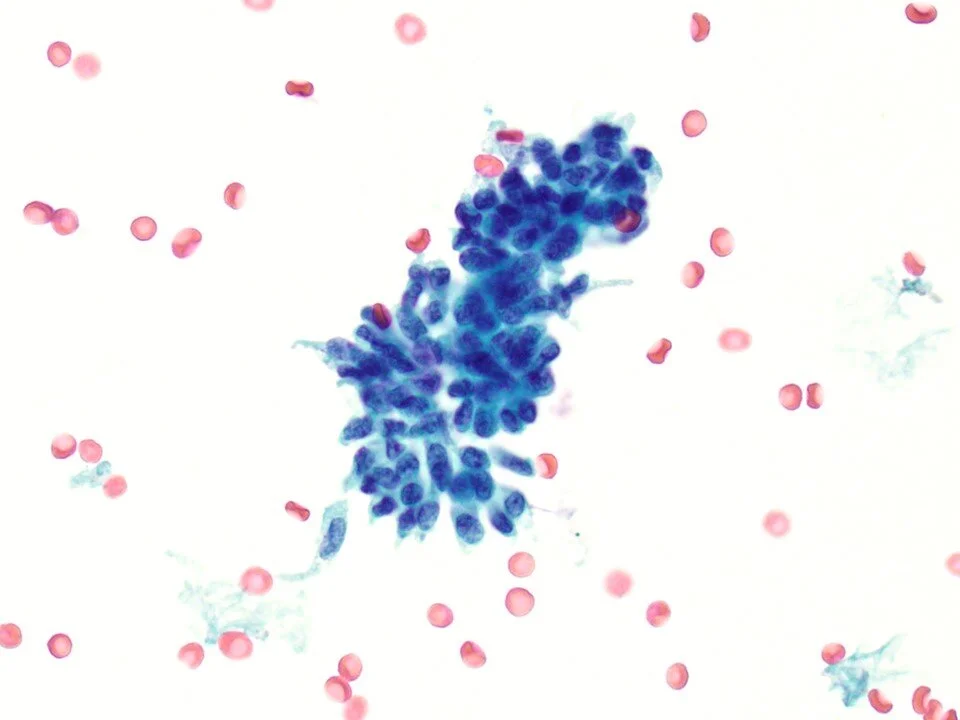
Some features include vacuolated polygonal cells with only mild nuclear atypia, including signet ring-like cells as seen here, cells forming papillary or loose groups, or isolated cells.
Don’t forget that not all cancers involving the bladder are primary urothelial carcinomas! Metastasis can occur.
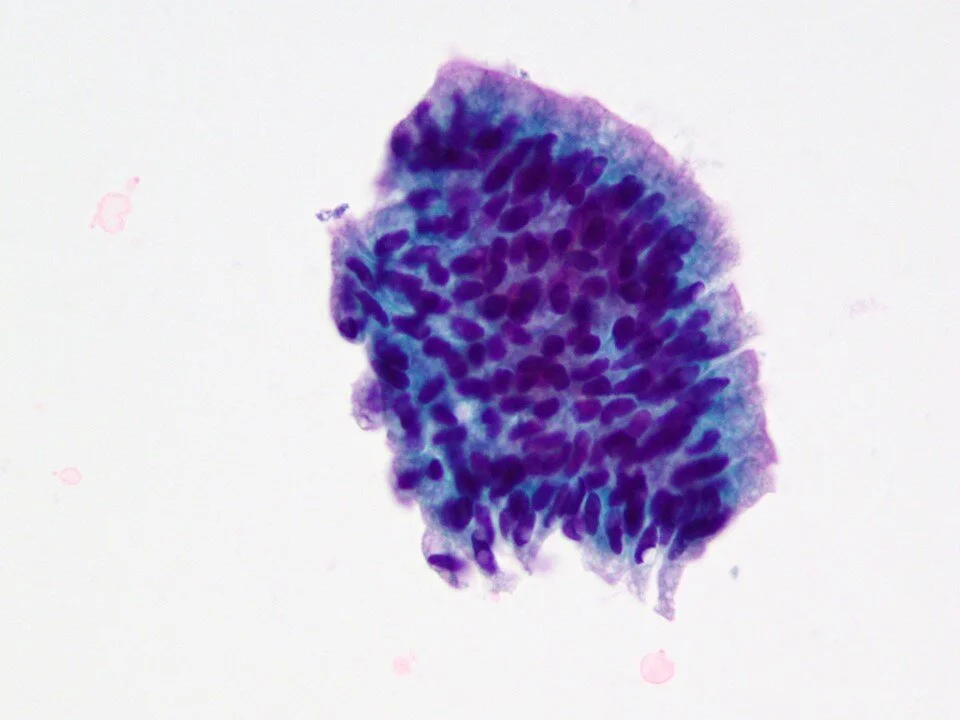
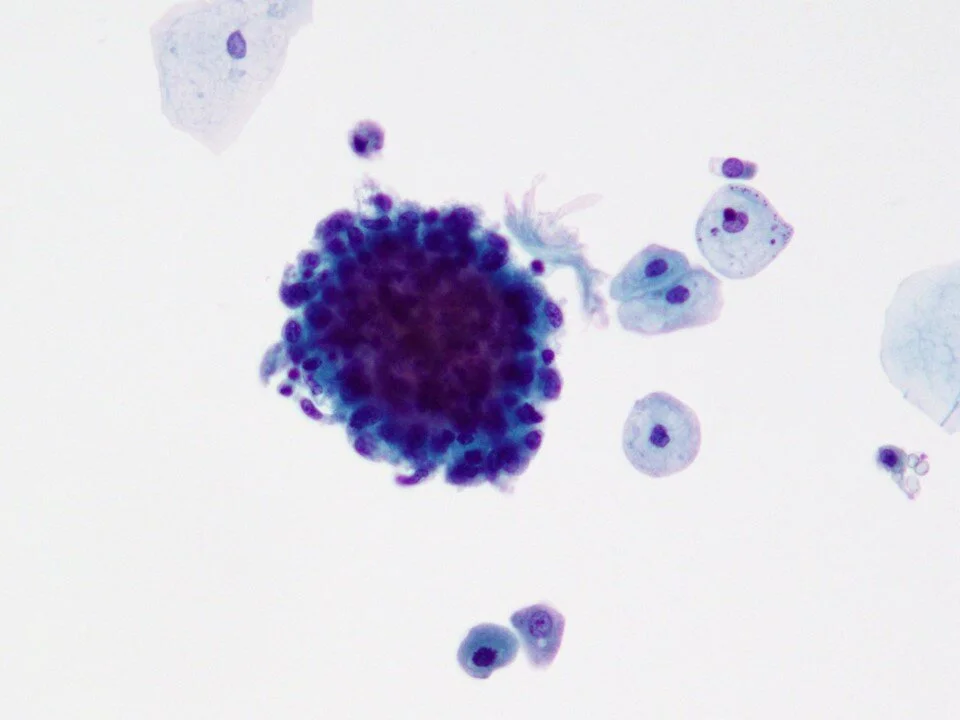
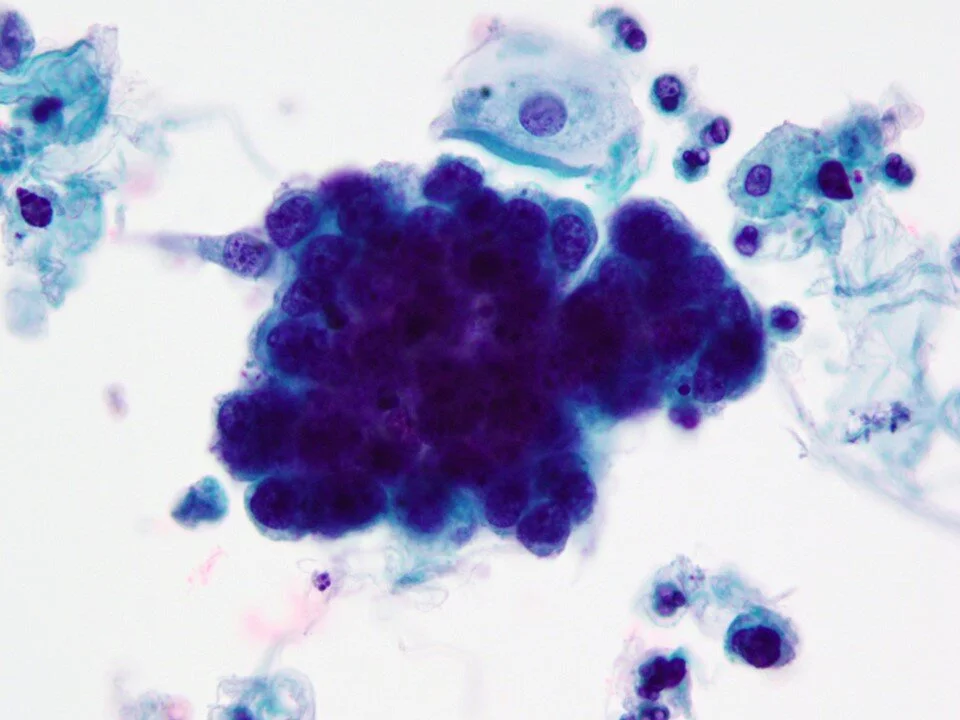
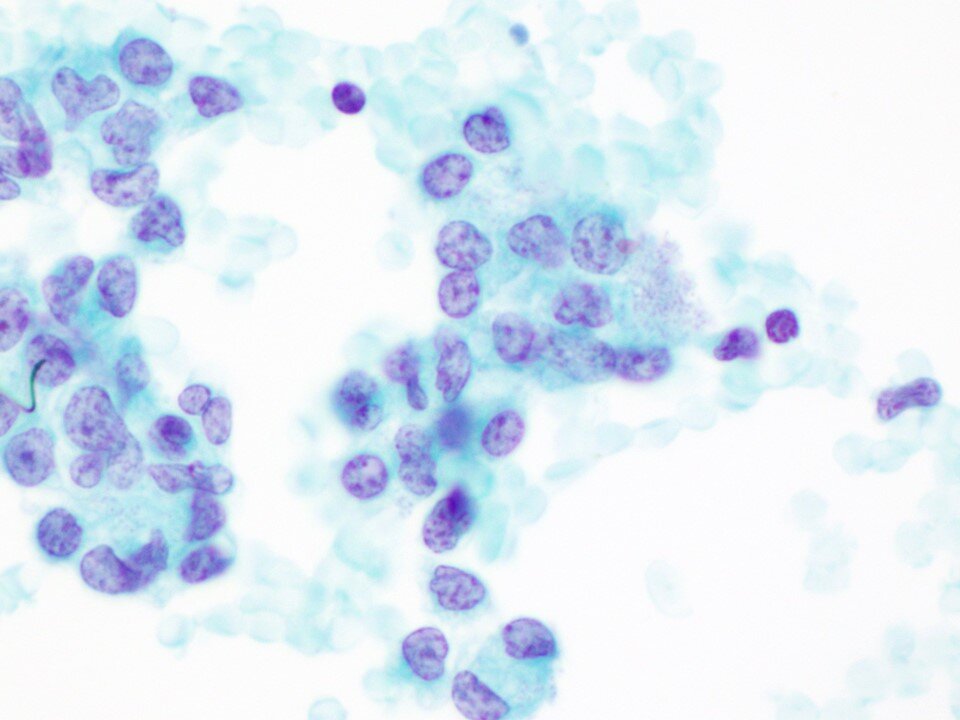
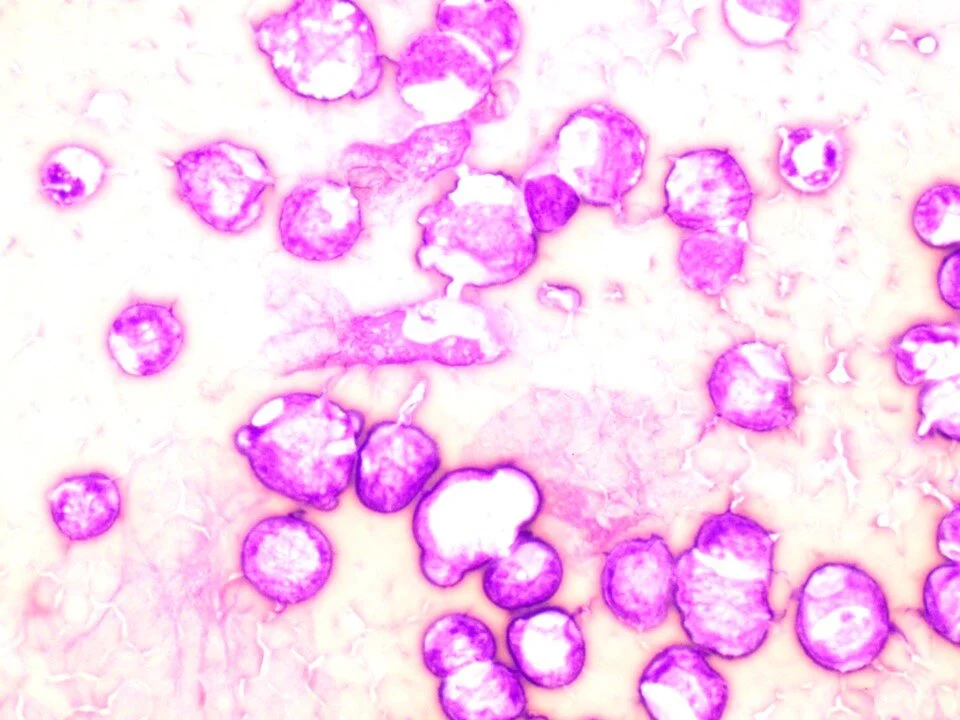
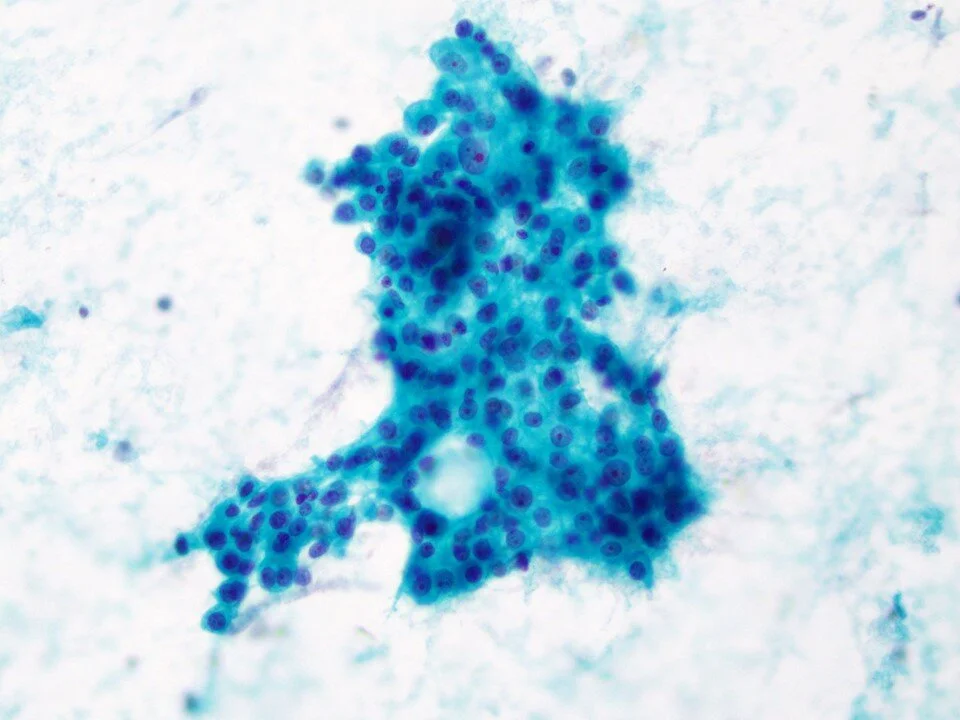
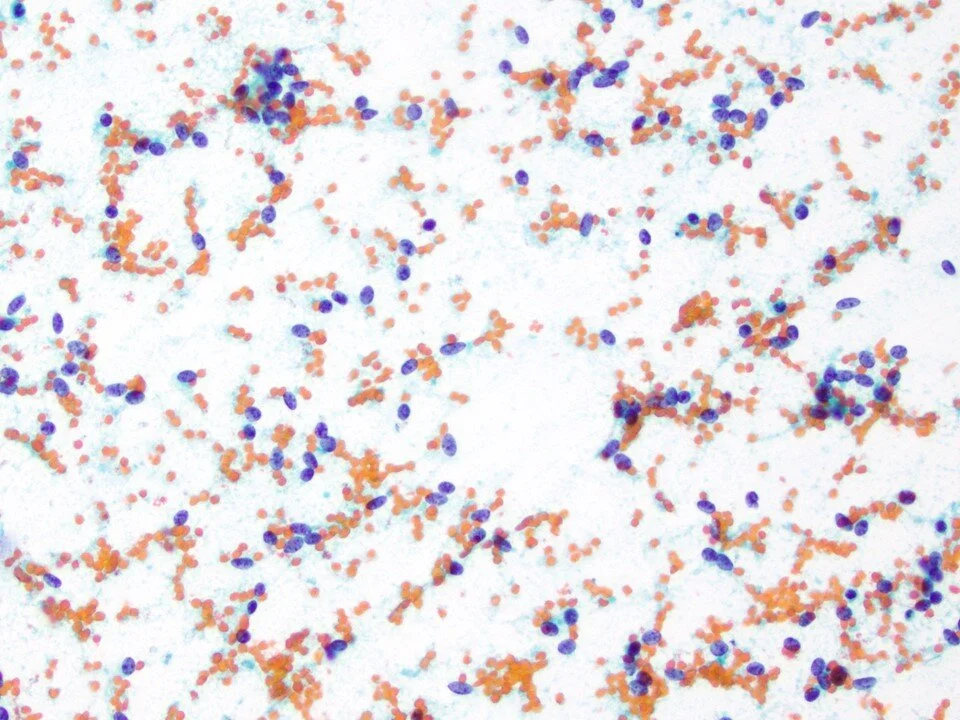
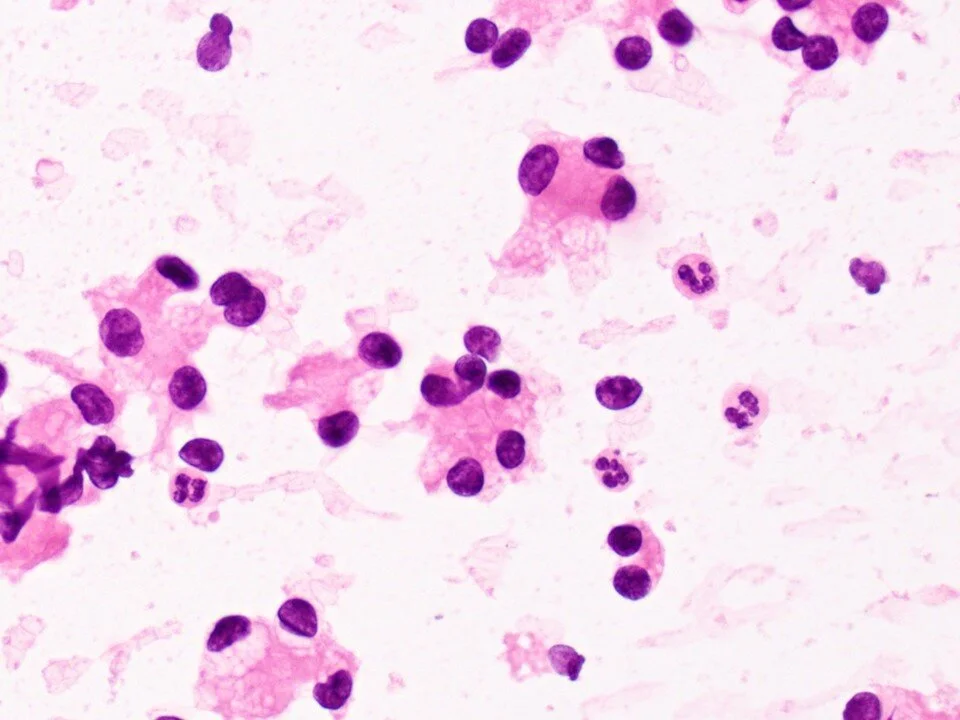
Small cell carcinomas are rare carcinomas of the bladder. They may be primary or secondary (often from the prostate). Note the especially high N:C ratio of these cells and the tight clusters (compare to the normal urothelial cells on the top left). Immunostains, including synaptophysin and chromogranin, can be helpful to point to neuroendocrine differentiation.
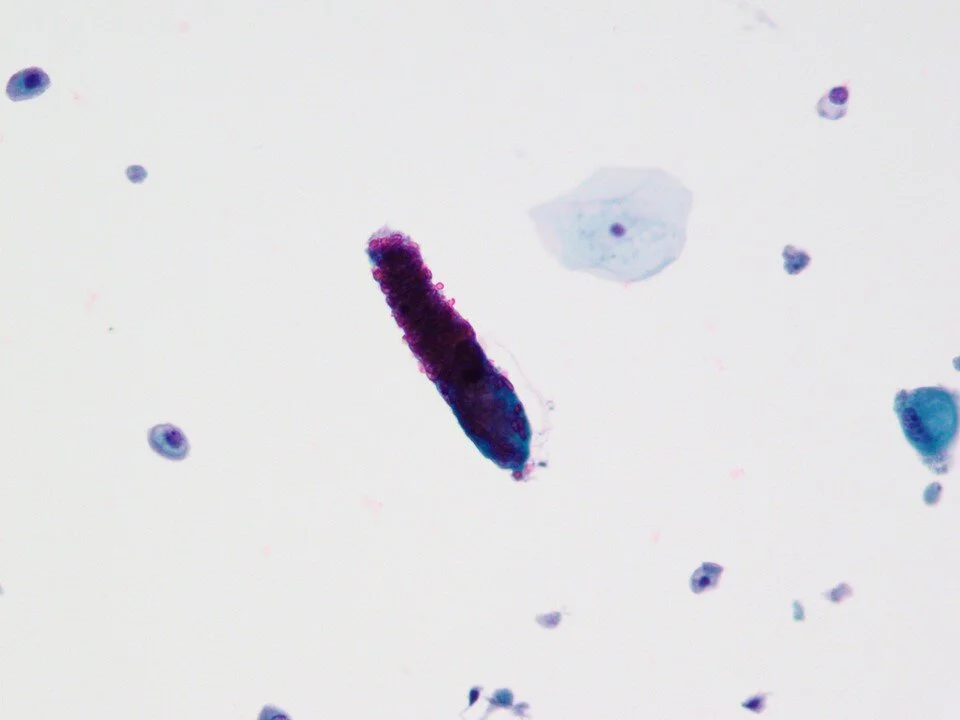
Bronchial epithelial cells (ciliated cells) and pulmonary macrophages (foamy cytoplasm). Pulmonary macrophages indicate that the distal airways have been sampled. Pulmonary macrophages can contain black carbon pigment as well as golden-brown hemosiderin pigment (indicating hemorrhage).
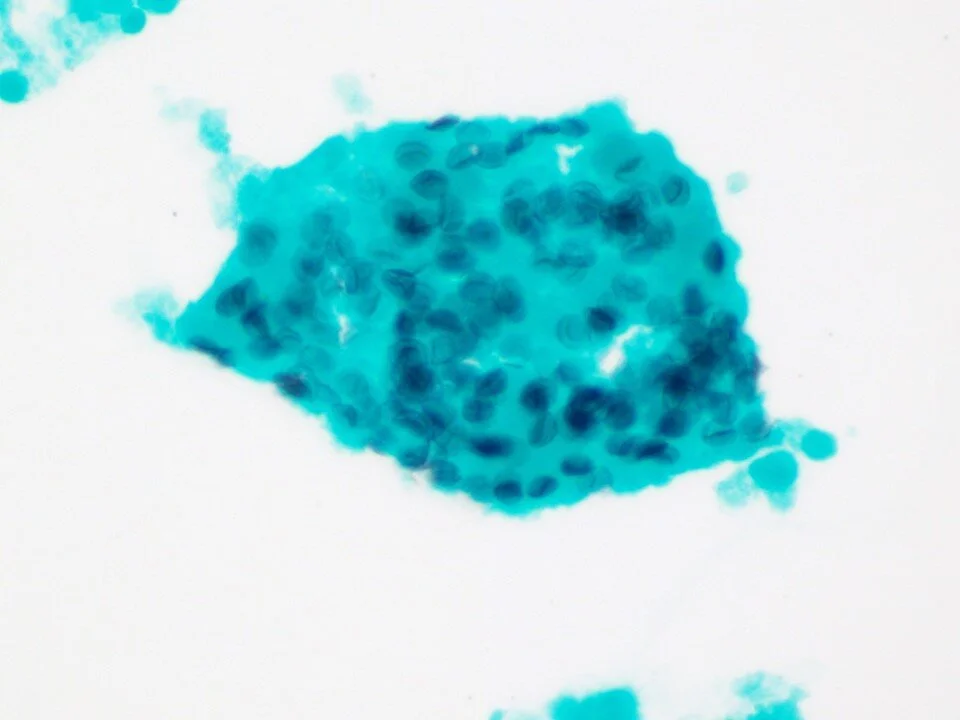
Reactive bronchial cells can be seen singly or in dense clusters such as this. They may be seen in dense clusters in chronic lung conditions such as asthma. These clusters may mimic those seen in adenocarcinomas; however, careful examination reveals cilia at the cell periphery.
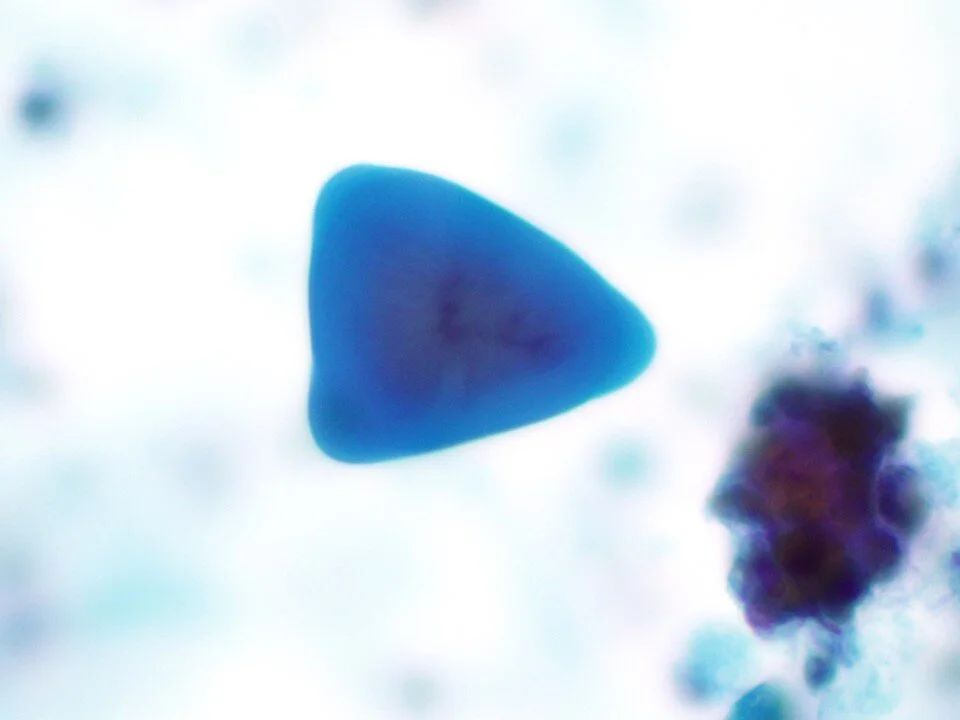
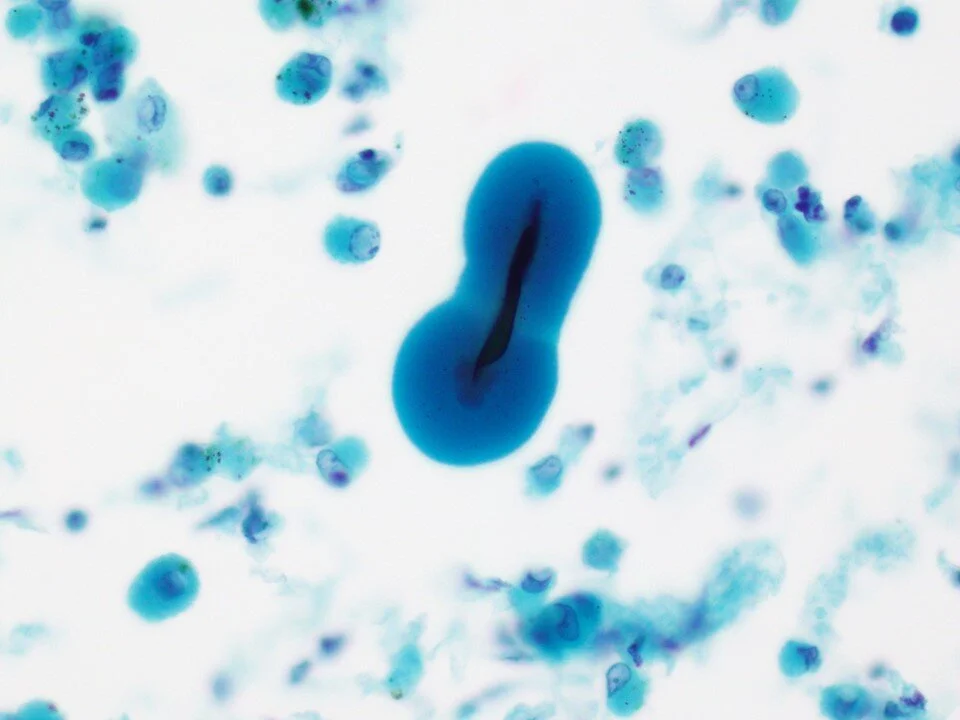
Corpora amylacea can be seen in BAL specimens such as in this case. They have no known significance. They may be angulated (as in this case) or more spherical (as in the next case below). Careful examination will demonstrate radiate striations or concentric laminations.
Some cases may also demonstrate central pigmented cores, as seen here.
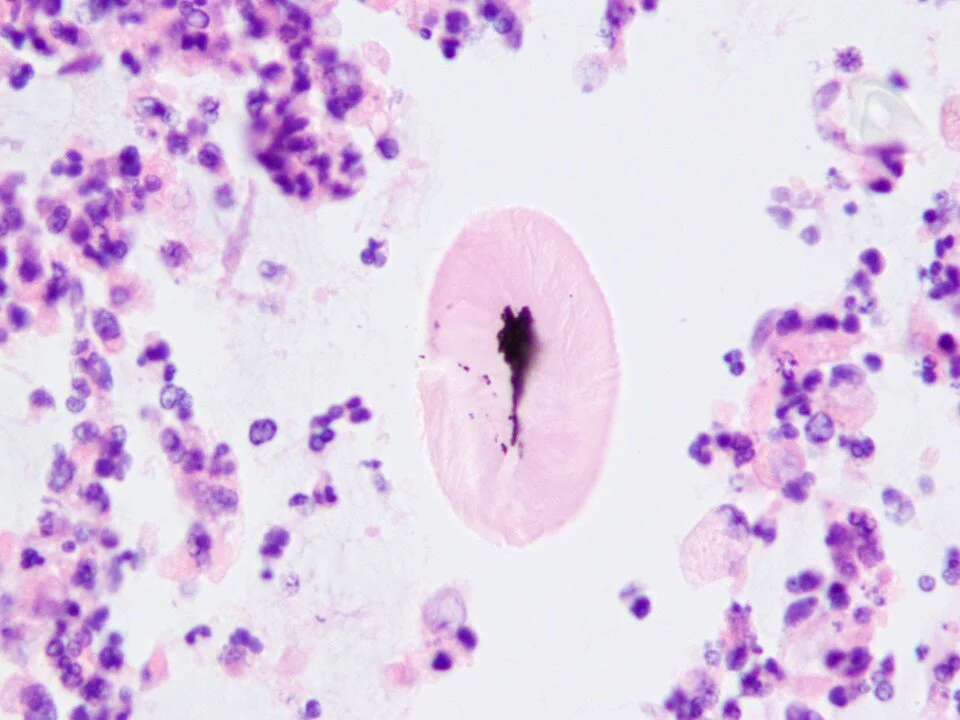
Cell block corresponding to the prior case, further demonstrating corpora amylacea with a pigmented core.
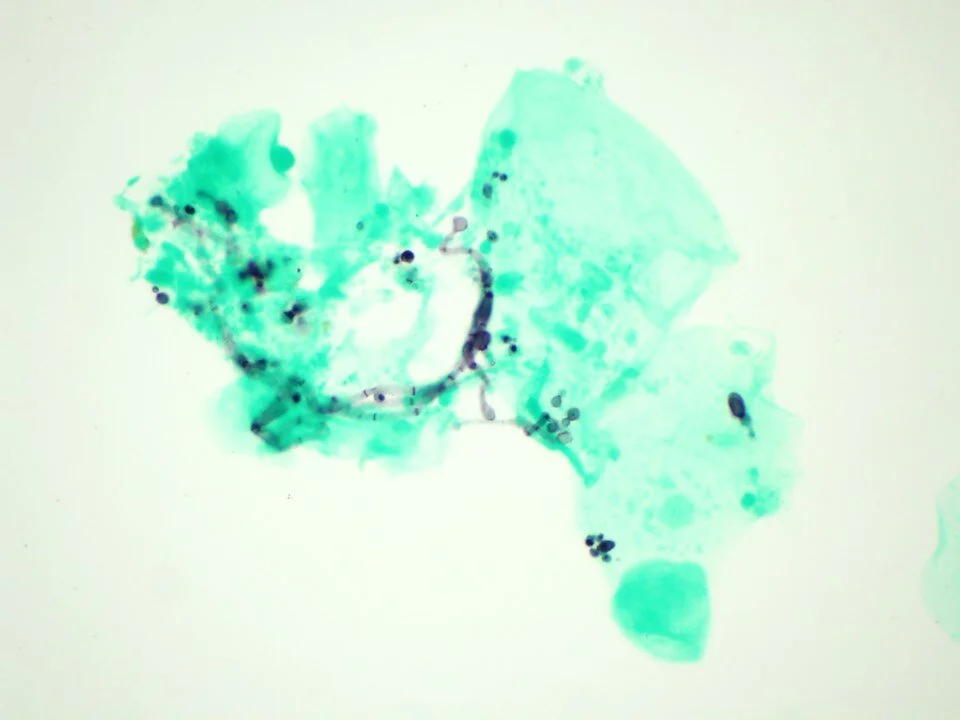
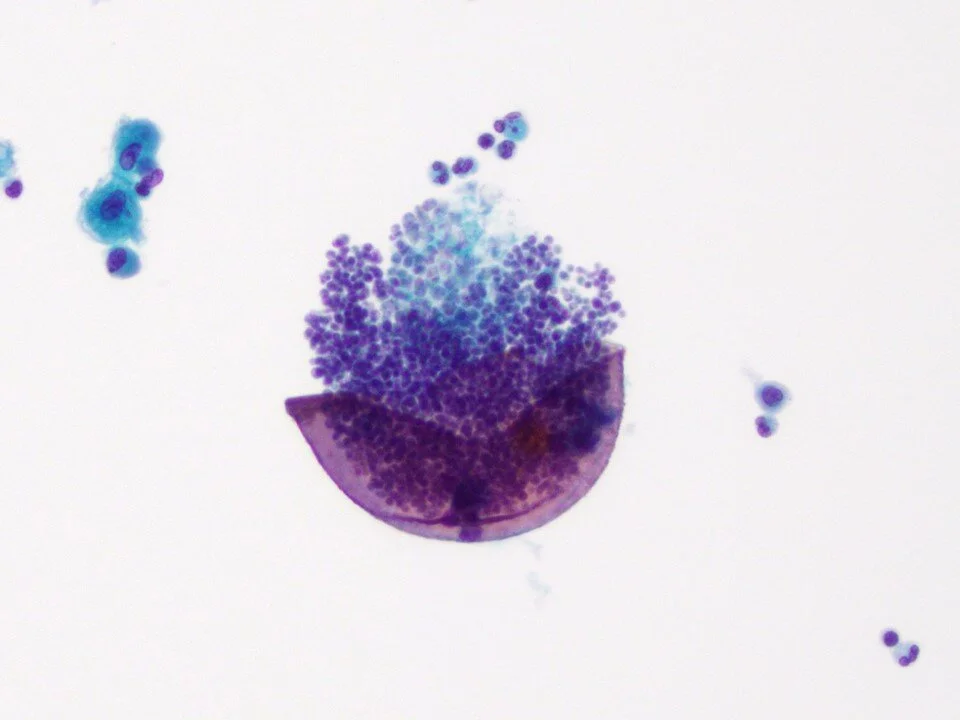
Pigmented fungus that is usually a specimen contaminant. Can be “snowshoe”-shaped as seen here, but also may be slender septate stalks or sometimes branched.
Ferruginous bodies are mineral fibers that are coated with a protein-iron-calcium matrix. They are golden-yellow to black in color and are dumbbell-shaped. Ones containing asbestos cores are referred to as asbestos bodies, which demonstrate a thin translucent core and may appear beaded. Iron / Prussian blue stains can highlight these bodies.
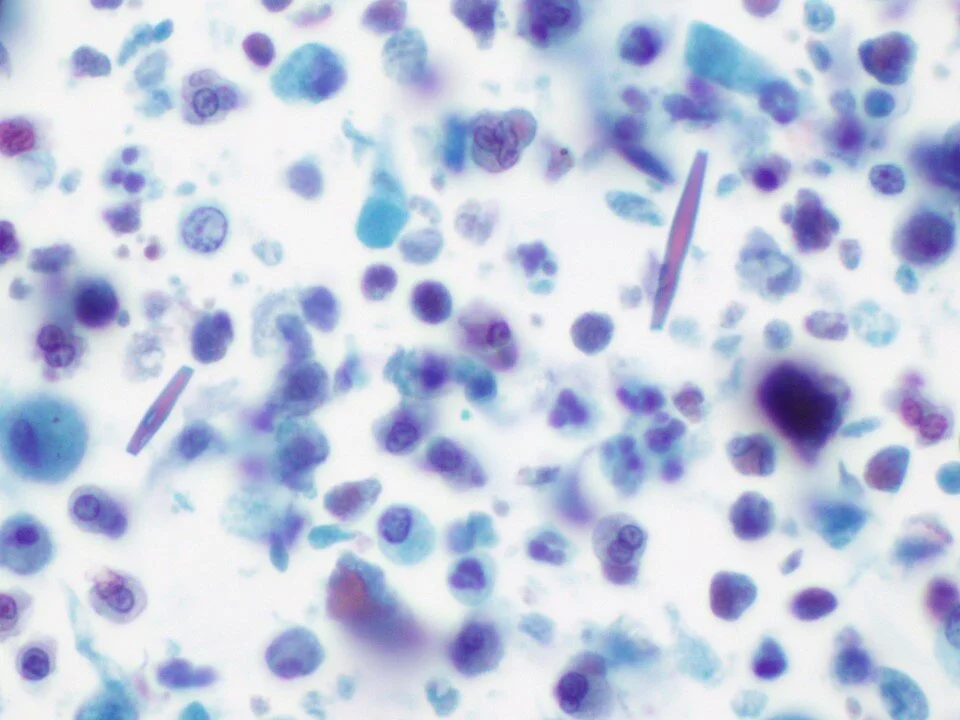
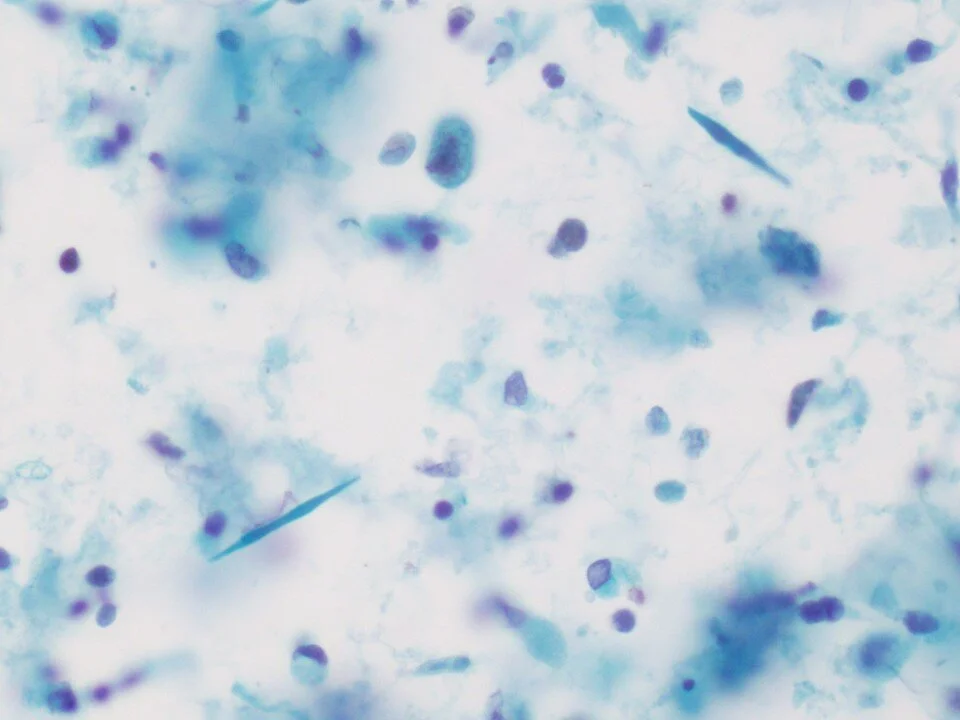
Needle to rhomboid shaped. A by-product of eosinophil degranulation. Thus, can be associated with allergic disorders like asthma or associated with fungal infection. This case was from a patient with aspergillosis.
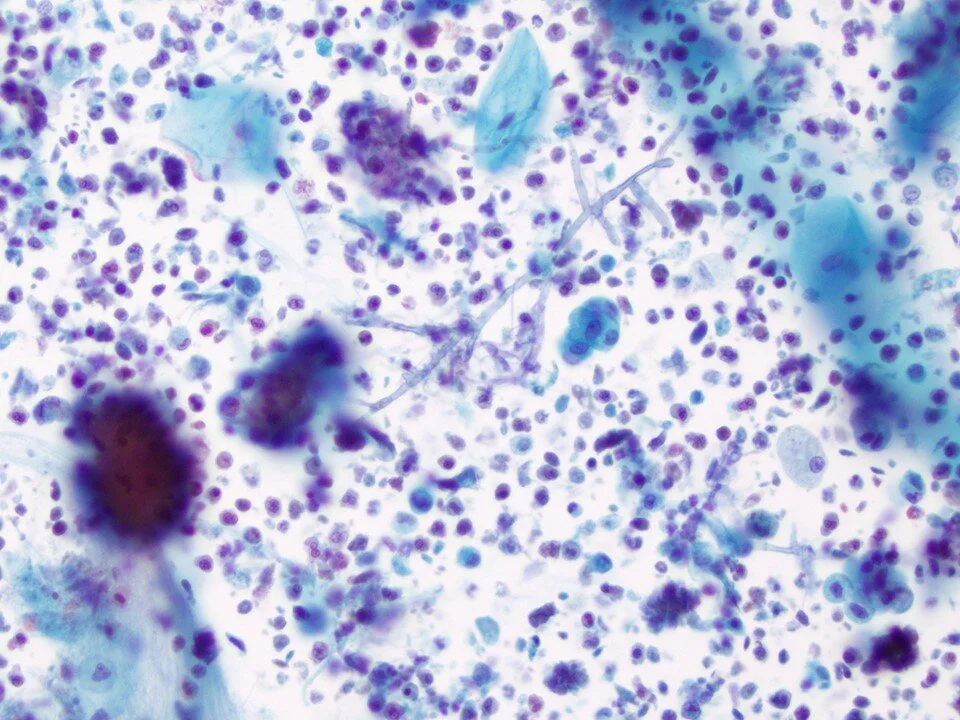
This case was also from a patient with aspergillosis.
Characterized by septate hyphae with 45-degree angle branching. Fruiting bodies may be seen in some cases, particularly when cavitary.
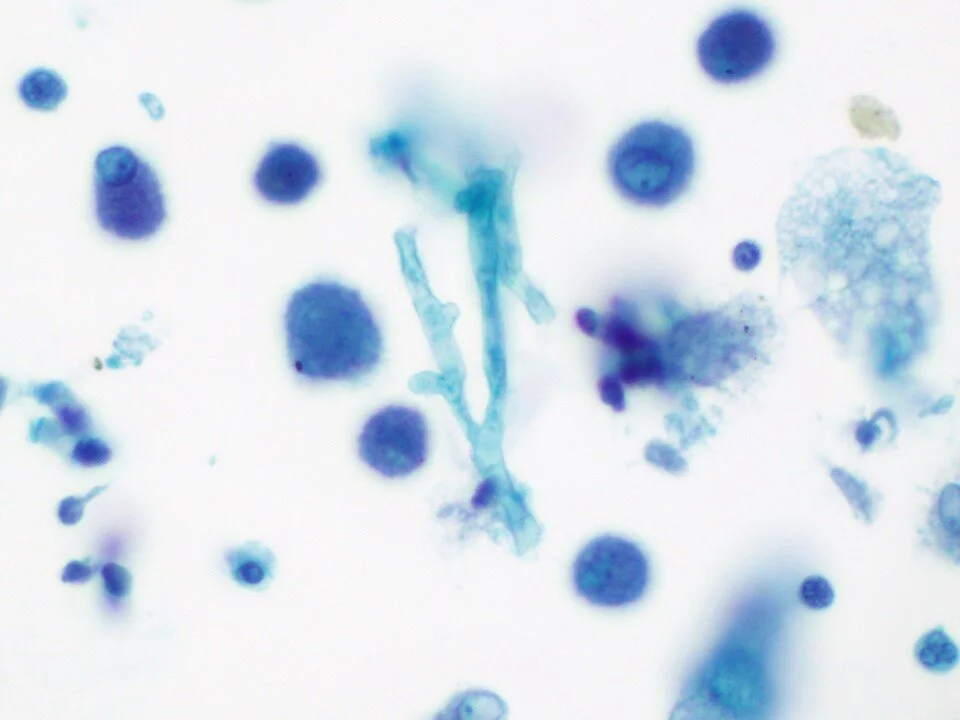
Note the acute / 45-degree branching and septated hyphae.
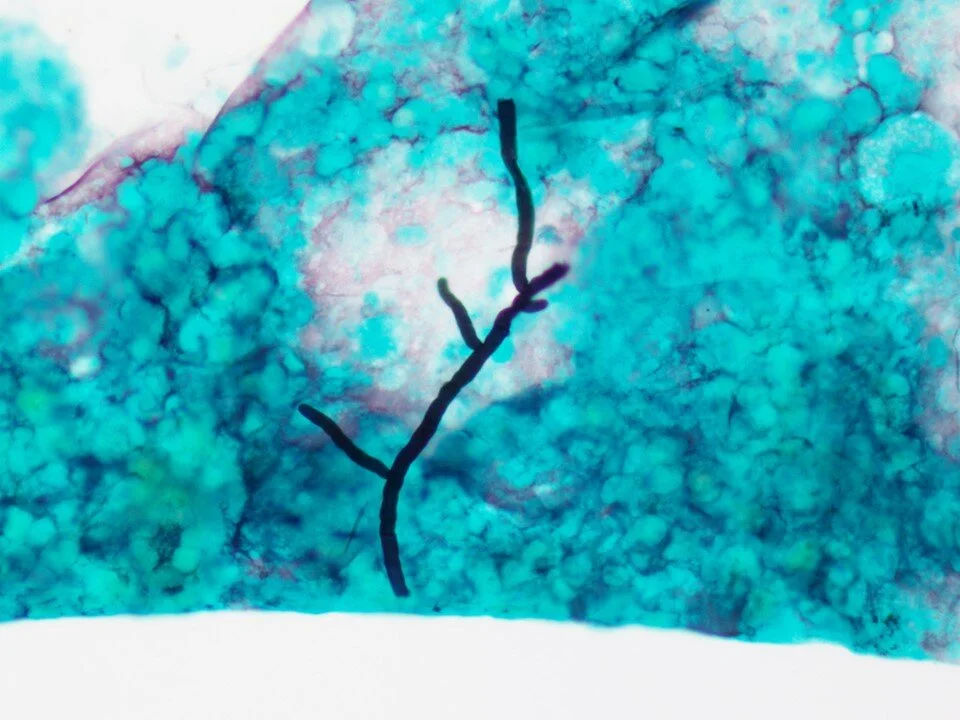
A GMS silver stain nicely highlights this case.
This fungus is characterized by budding yeast forms and “pseudohyphae” which are formed from the budding yeast not pinching off from one another (imagine sausage-links).
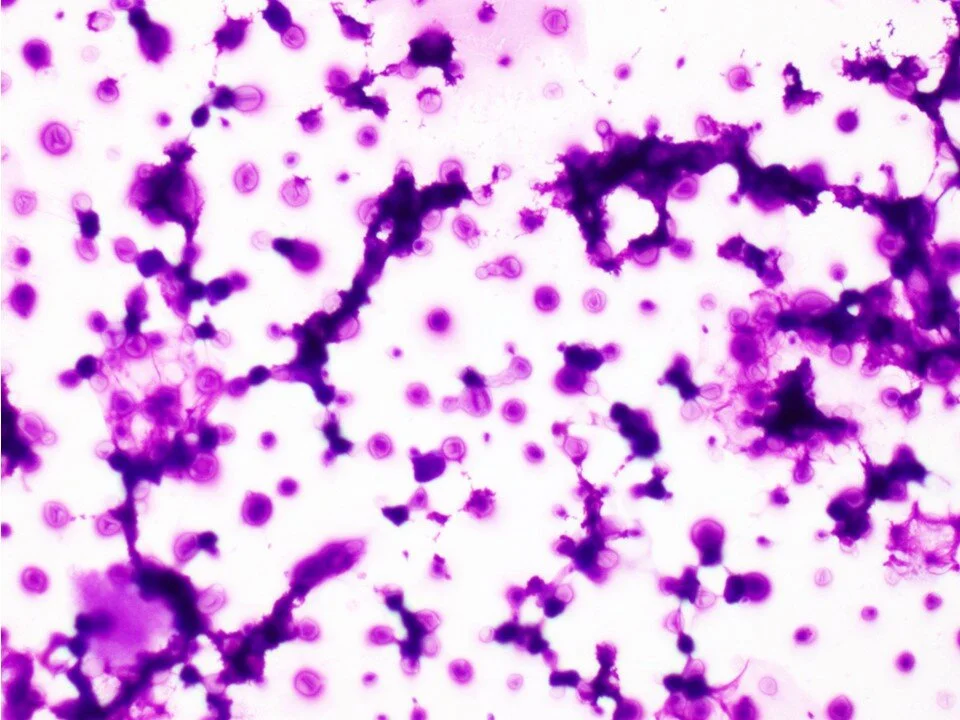
Now considered a fungus, this organism is not visualized on Pap staining. However, they can be seen within circumscribed froathy-appearing proteinaceous alveolar casts.
The organisms appear almost as negative images within the proteinaceous material.
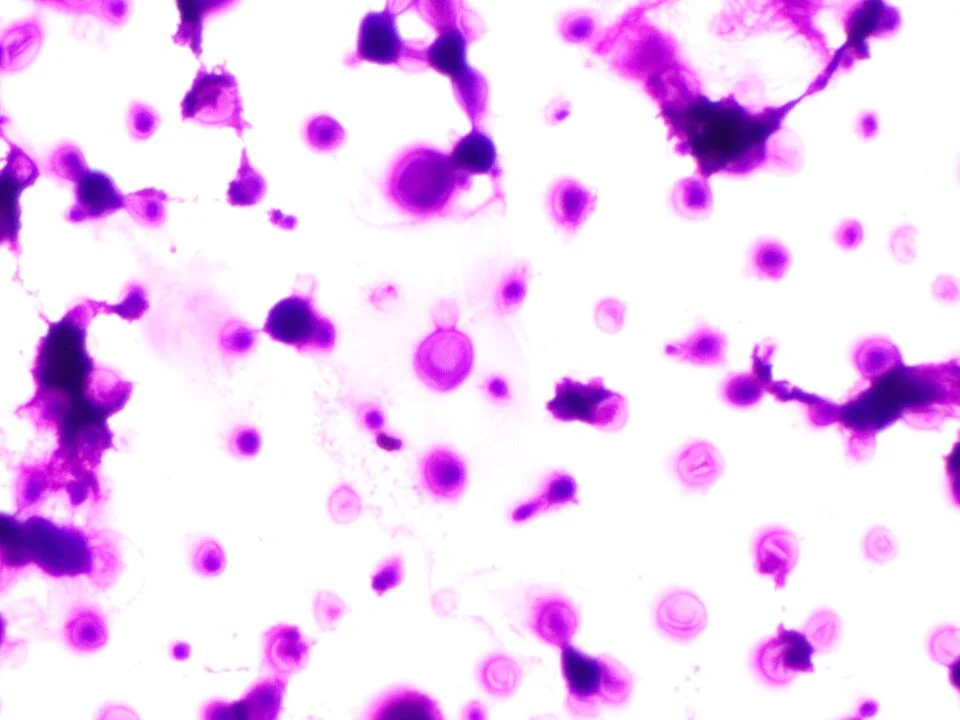
Another example
A GMS stain highlights the cup-shaped fungal organisms. Note that there is no budding seen with this fungus unlike others in the differential.
Dimorphic fungus characterized by spherules that can fracture and release endospores. The hyphae (as seen here) are only rarely seen.
Ruptured spherule releasing endospores
A central parent yeast with budding yeast forms imparts a classic “mariner’s wheel” appearance of this fungus.
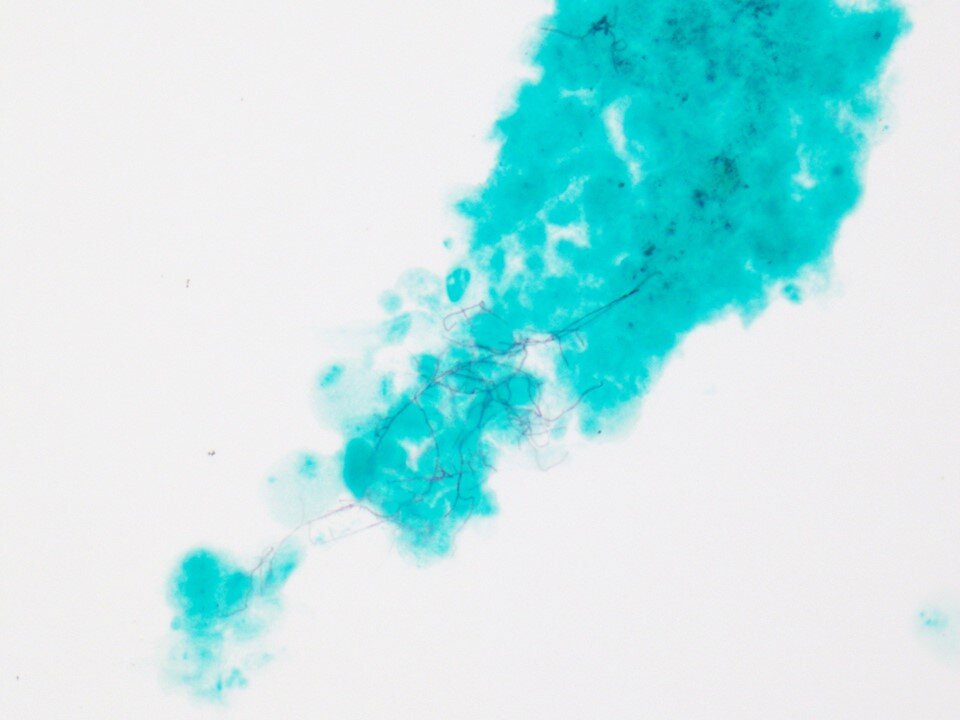
GMS stains, while classically used to highlight fungal organisms, can also pick up other organisms. In this case, the GMS stain highlighted Nocardia bacterial organisms.
Reference: https://pubmed.ncbi.nlm.nih.gov/31043291/
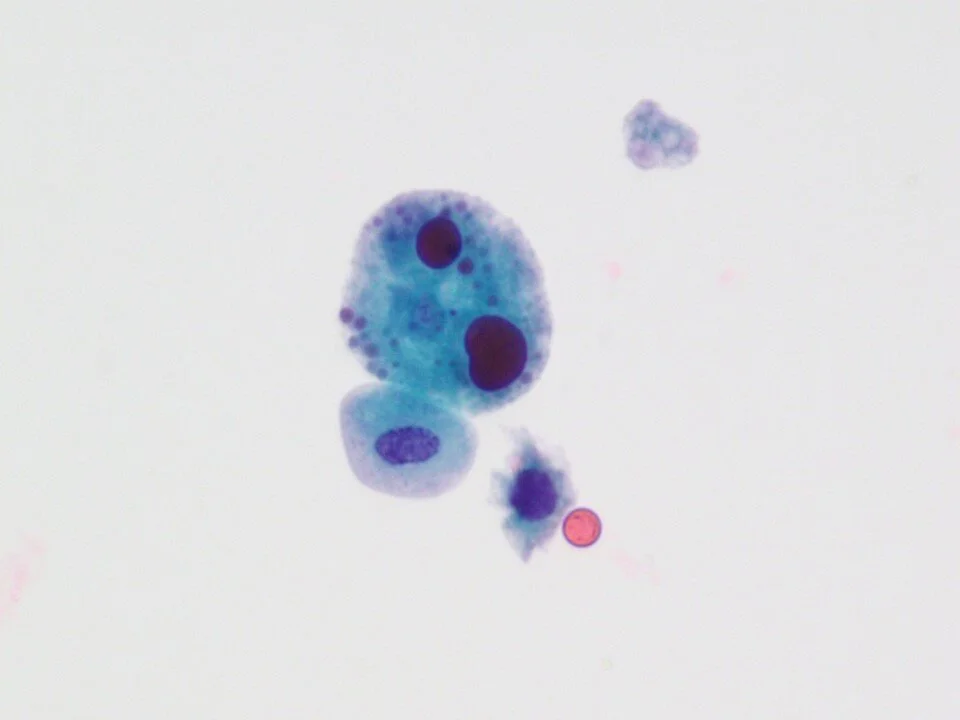
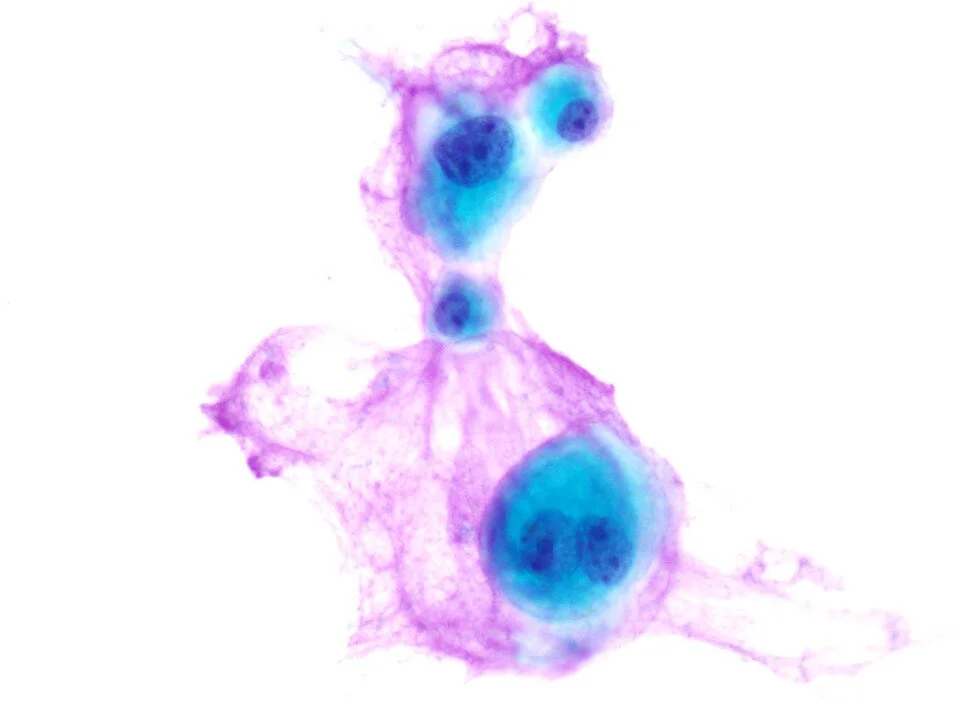
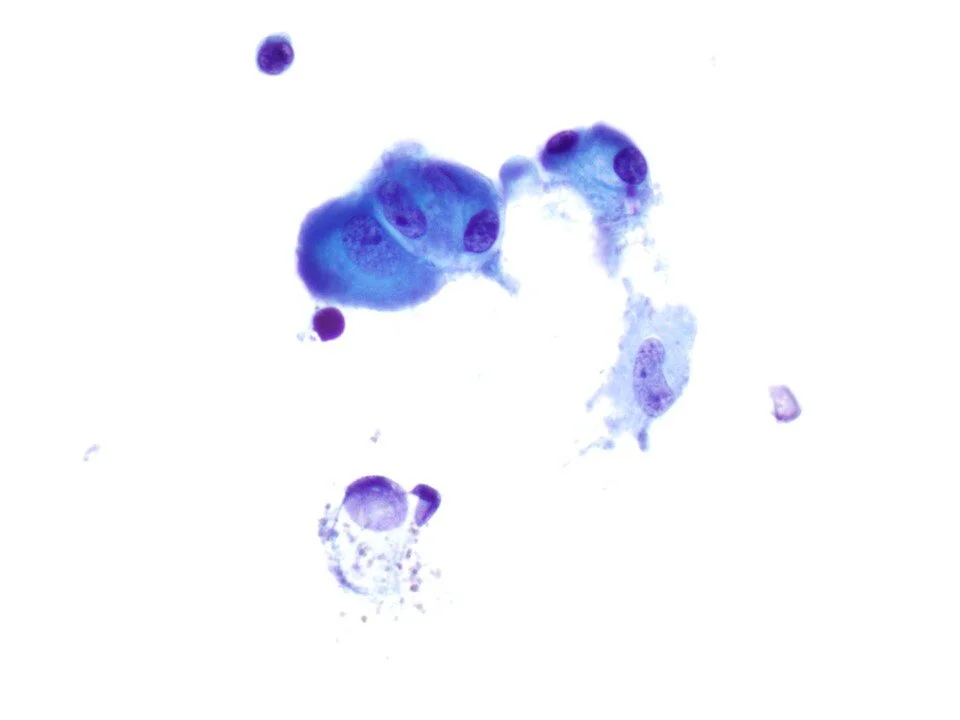
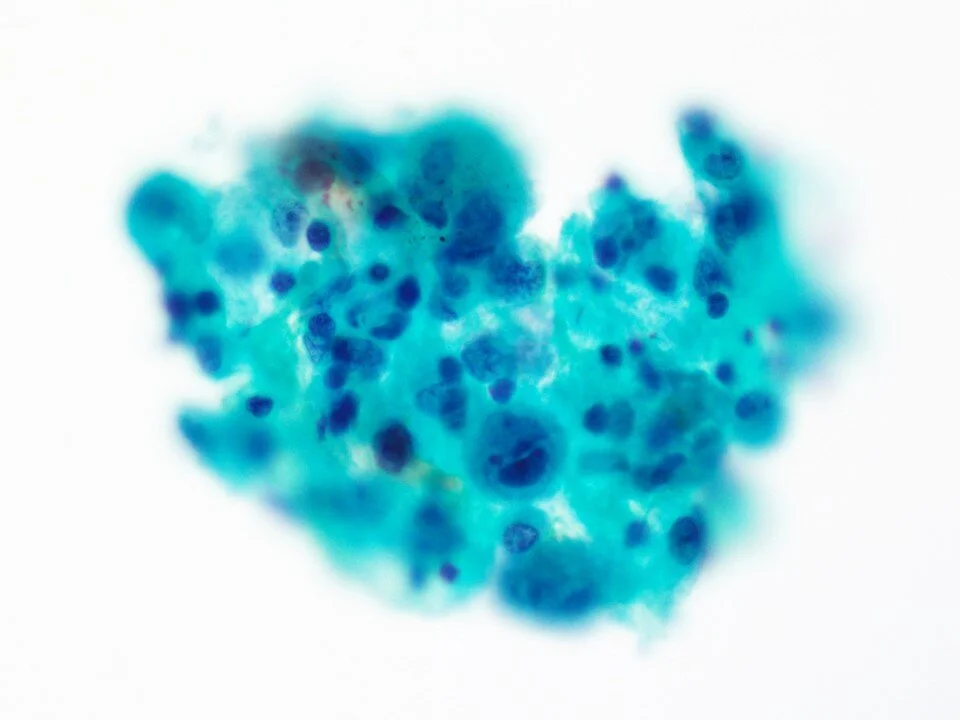
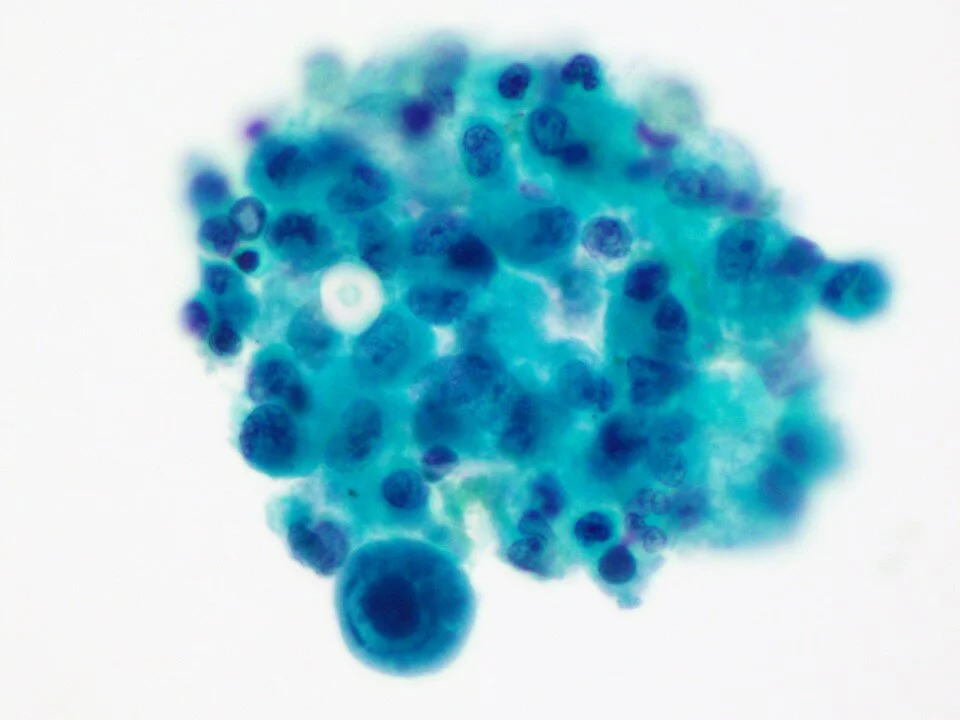
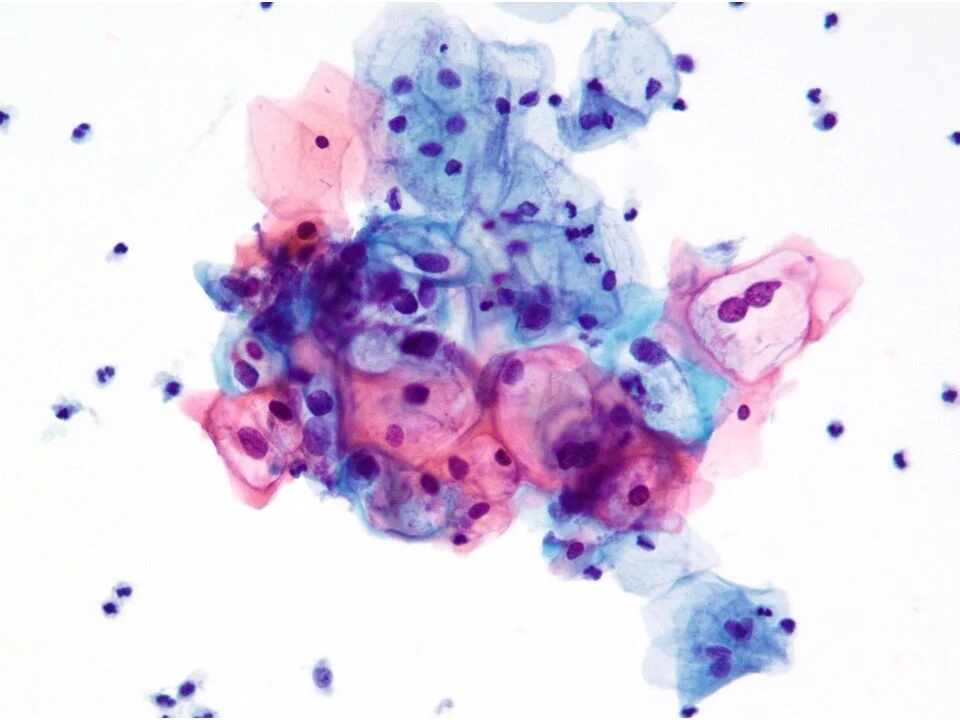
Most commonly affects immunocompromised patients. Can involve the pharynx, larynx, tracheobronchial tree, or pulmonary parenchyma. Viral cytopathic changes include the 3 M’s: multinucleation, molding (of nuclei), and margination (of chromatin). The viral particles impart a glassy look to the nuclei (as seen in this case). Well-circumscribed eosinophilic (Cowdry A) nuclear inclusions can be seen in some cases.
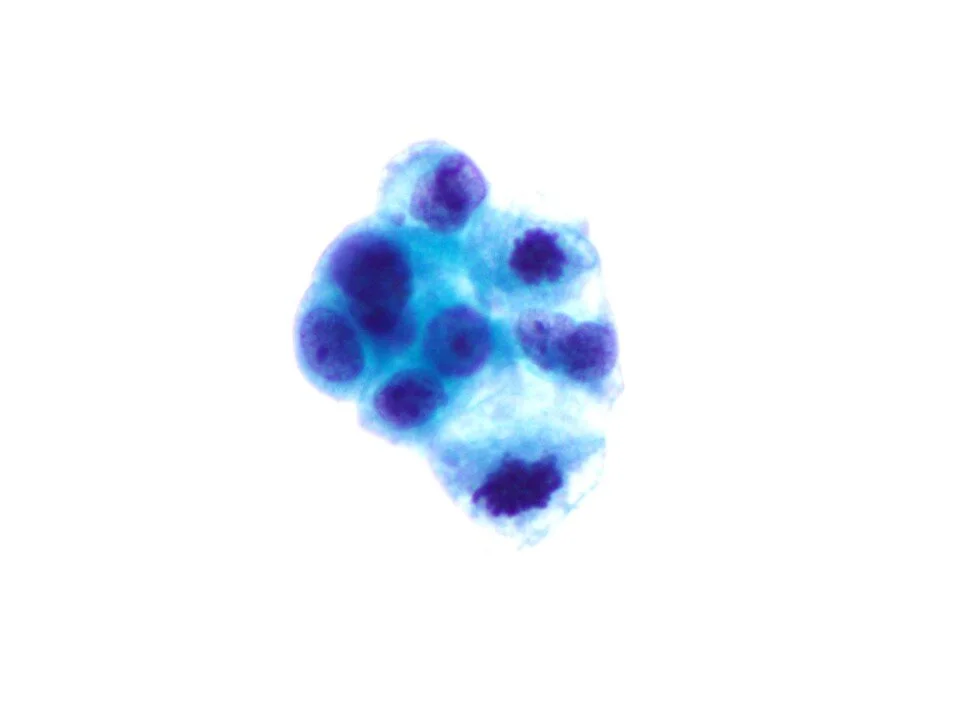
Viral cytopathic changes include cytomegaly, large basophilic nuclear inclusions, and small basophilic cytoplasmic inclusions.
Viral cytopathic changes can be seen in bronchial cells, pneumocytes, macrophages, endothelial cells, or fibroblasts.
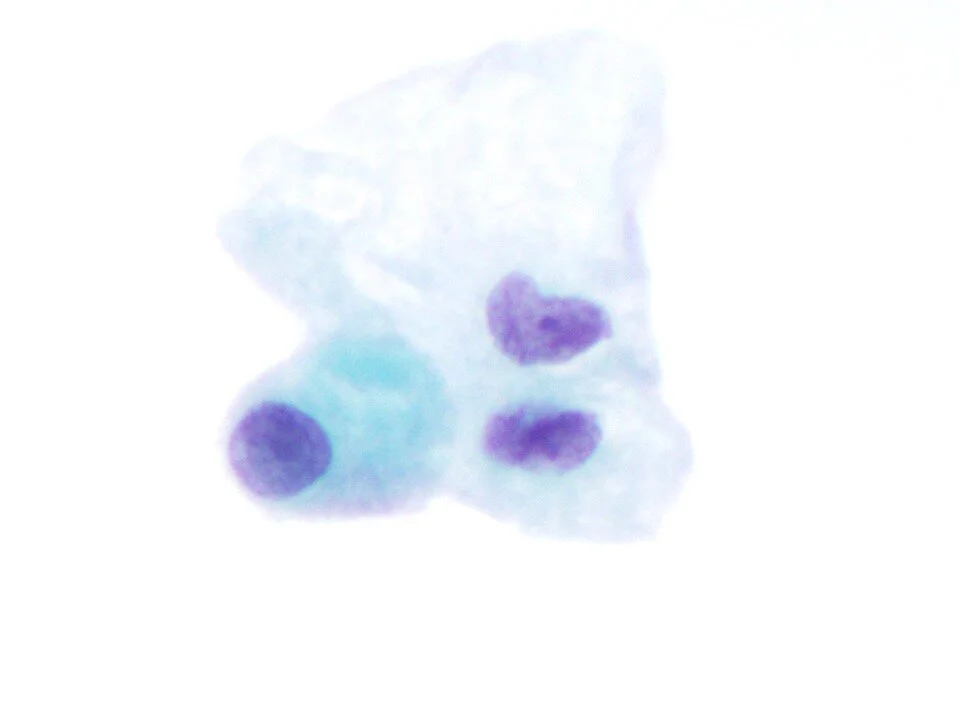
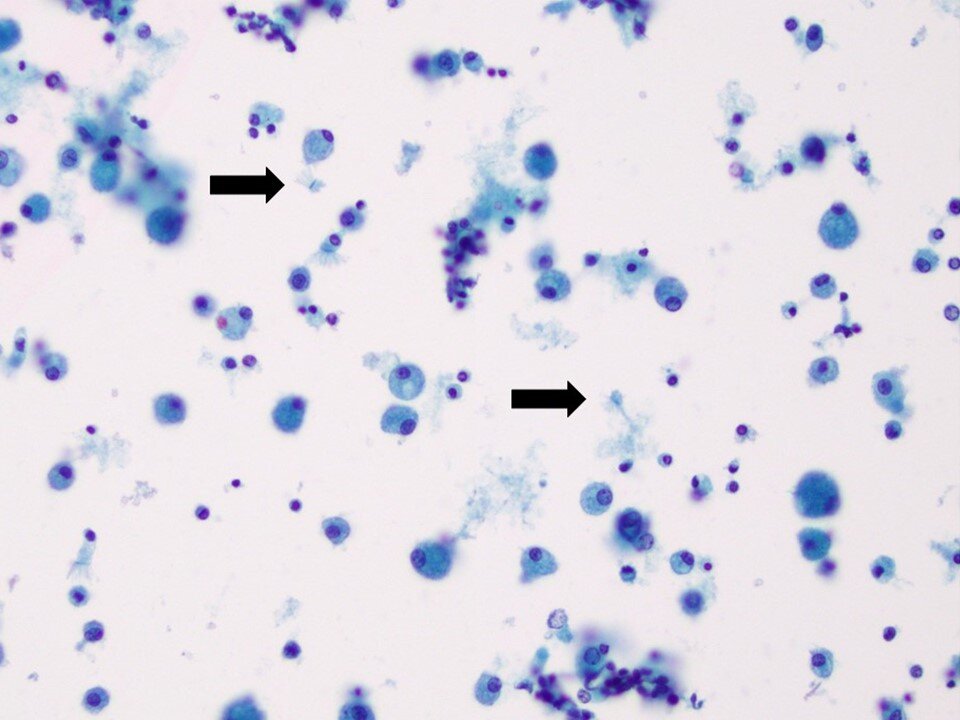
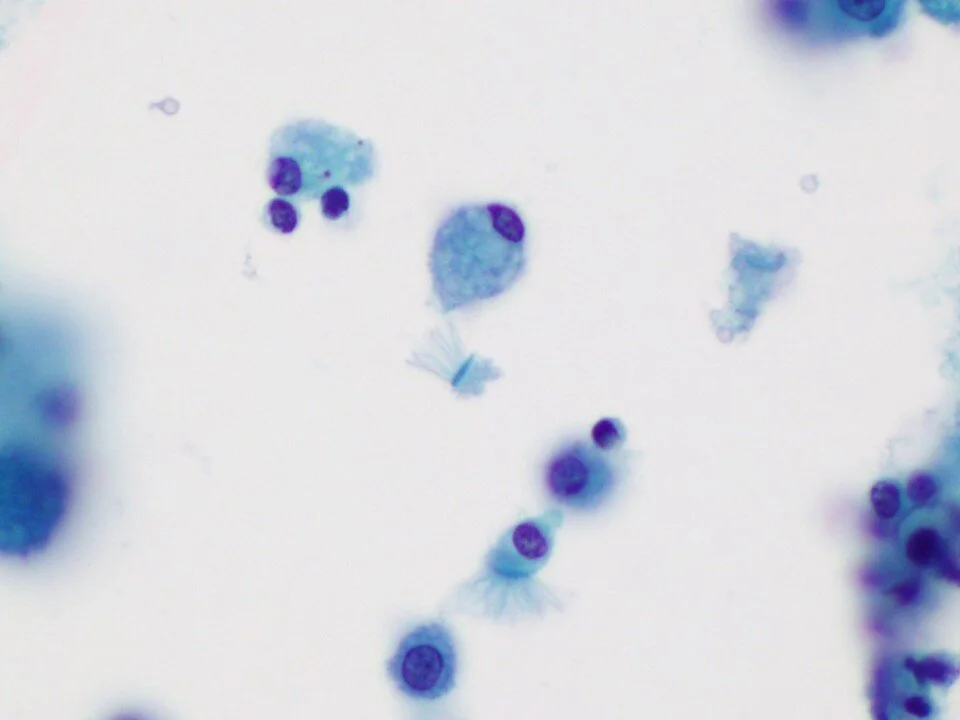
A distinctive type of cellular degeneration of bronchial epithelial cells that has been associated with viral (past or present) infection. While somewhat non-specific to the viral type, it has been associated with Adenovirus infection among others.
A distinctive form of degeneration of bronchial epithelial cells where the ciliated tuft becomes detached.
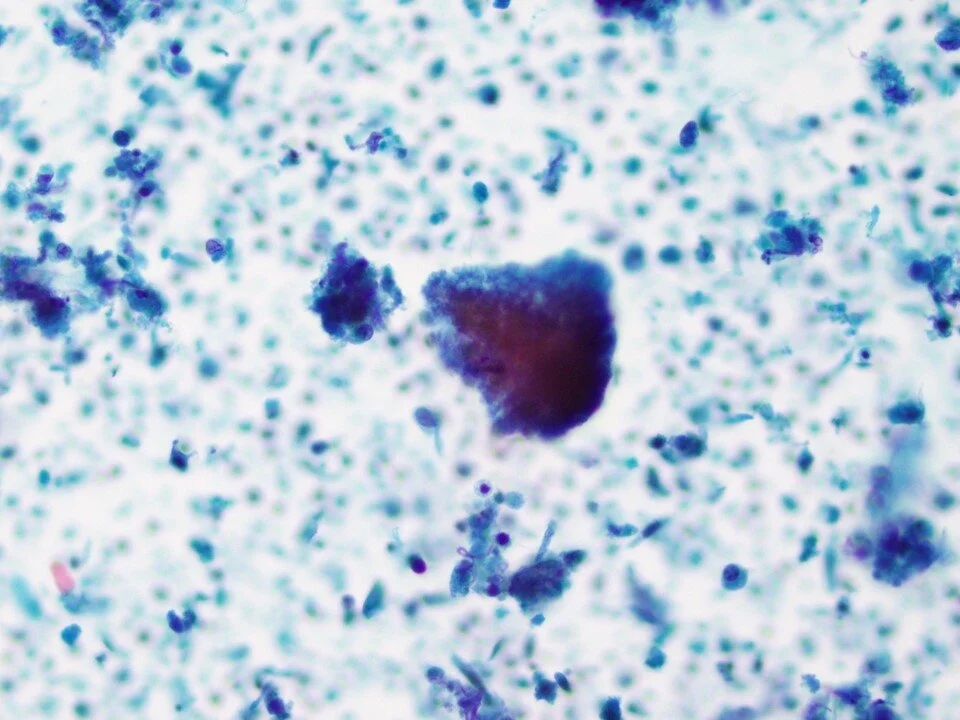
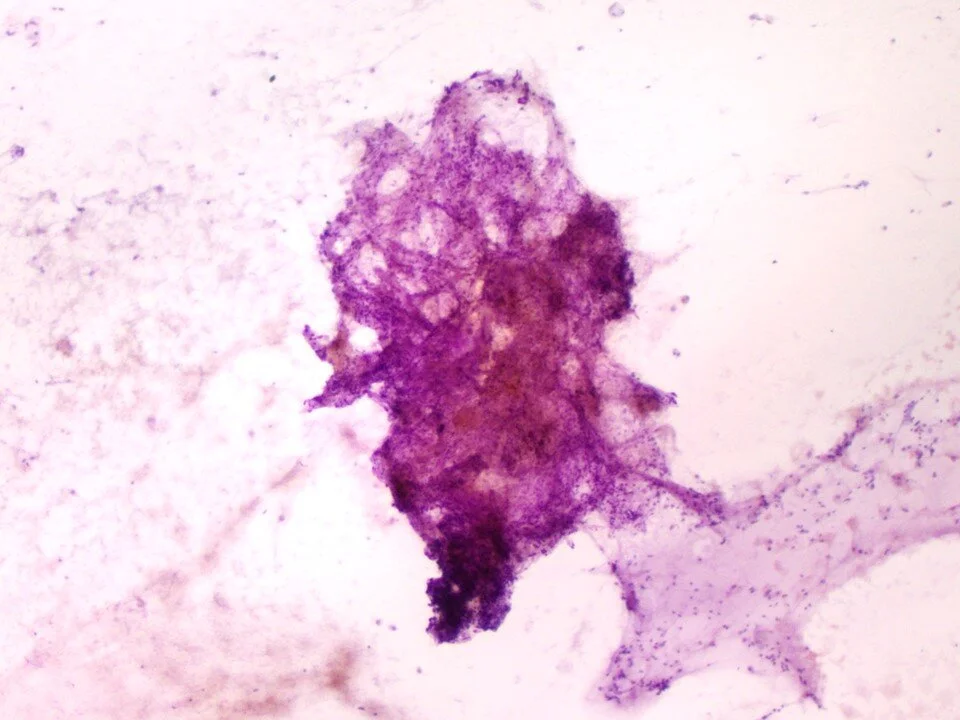
Large crushed tissue fragments may be seen in organizing PNA. These are composed of fibroblasts and collagen which fill the alveolar masses and thus take on a nodular appearance (Masson bodies).
Organizing PNA is characterized by fibrous tissue, pulmonary macrophages +/- hemosiderin, lymphocytes, and pneumocytes. The findings are not totally specific, and thus clinical correlation is needed to ensure that a lesion is not being undersampled.
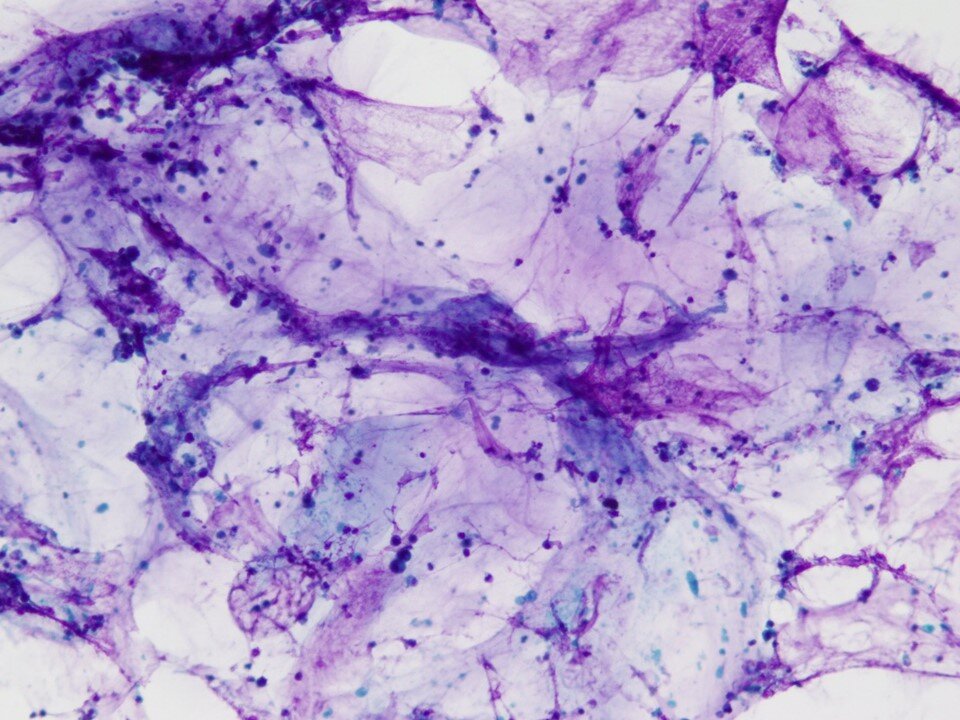
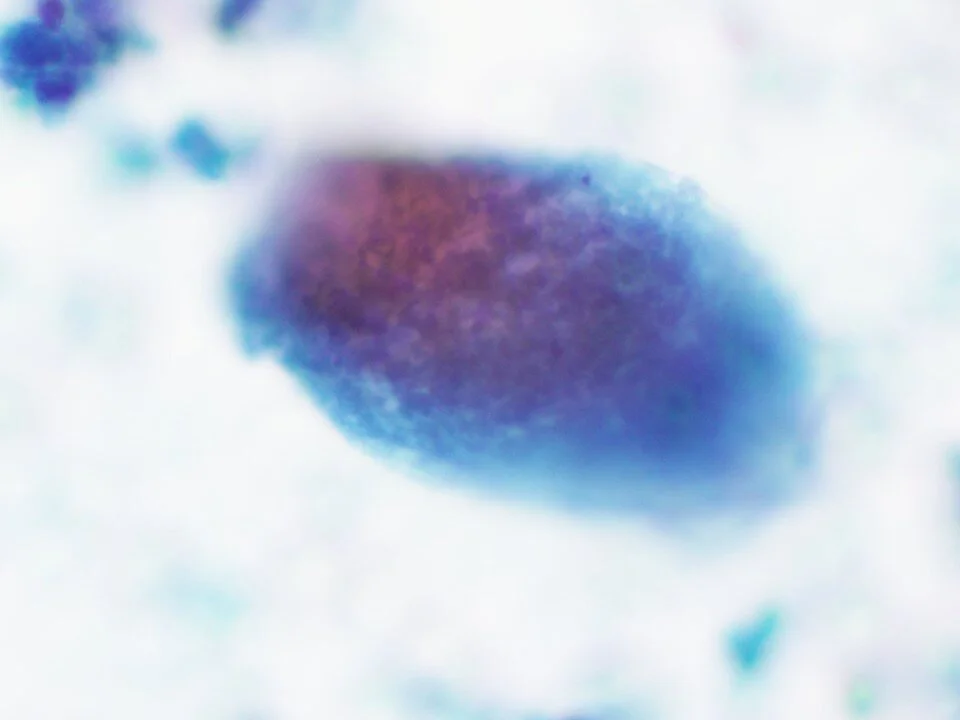
PAP is characterized by the accumulation of lipid-rich material within the alveolar spaces and thought to be secondary to macrophage dysfunction.
Cytologically, identified are acellular eosinophilic aggregates.
The eosinophilic “blobs” are PAS positive.
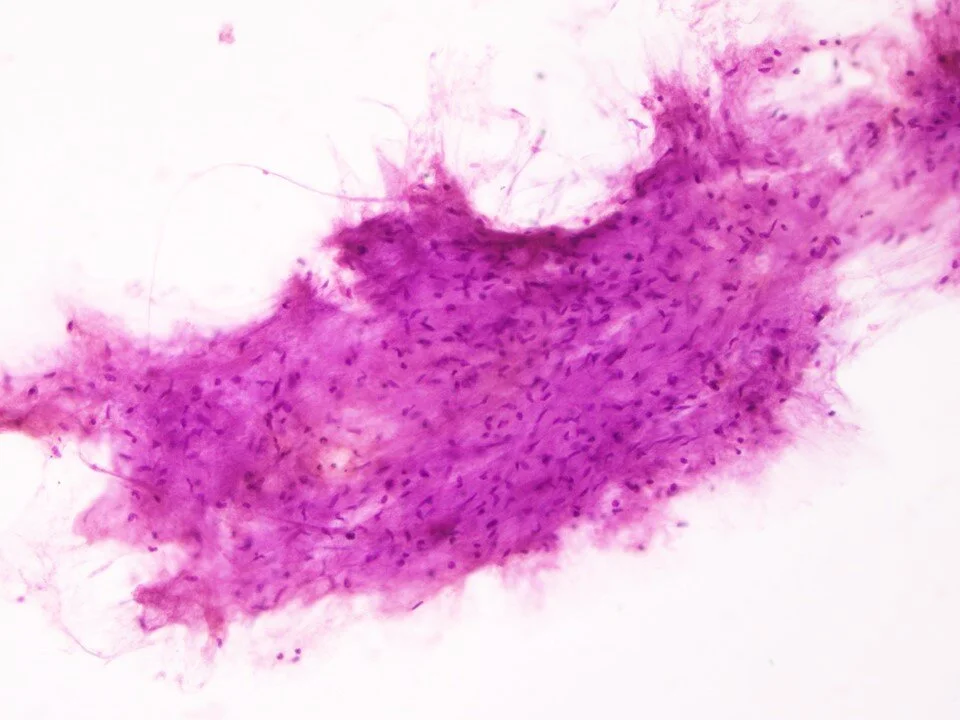
Pulmonary “hamartomas” are in actuality neoplasms (having been found to have recurrent clonal rearrangements involving the HMGA1 gene). On radiology, they are classically identified as well-circumscribed peripheral lesions. On microscopic examination, components that can be identified are benign glandular cells, fibromixoid matrix and bland spindle cells, cartilage with chondrocytes, and adipocytes.
Immature fibromyxoid material and bland spindle cells.
Bland glandular cells.
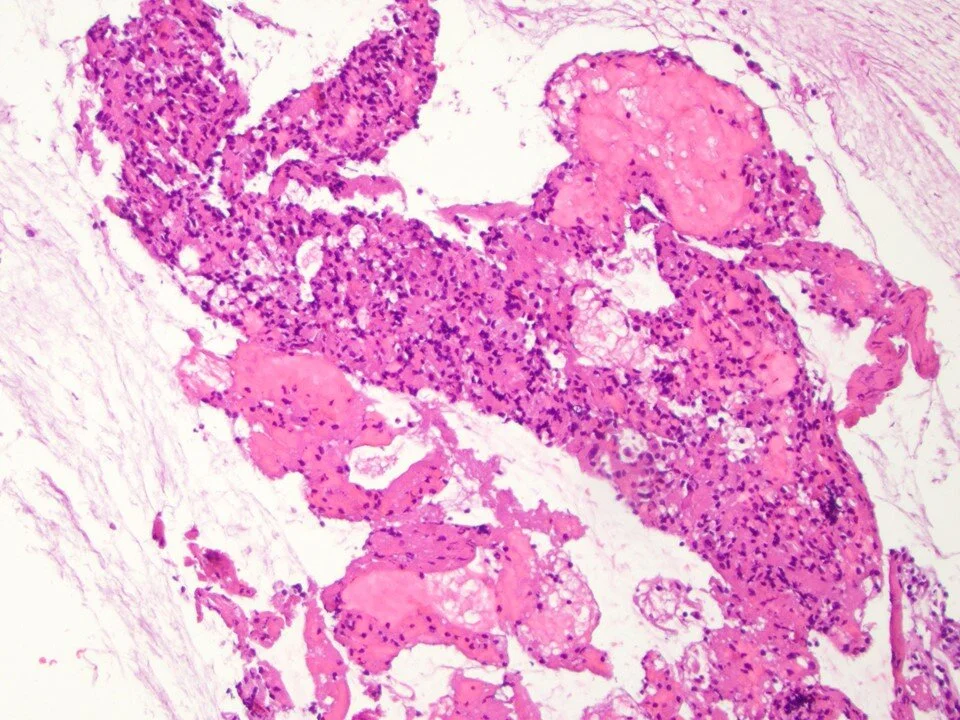
Rare benign tumor of the lung. Usually found in peripheral lung as a well-defined solitary rounded to oval mass. Microscopically, can see several patterns (papillary, sclerotic, solid, hemorrhagic).
Cells are rounded to polygonal with abundant eosinophilic cytoplasm. Cytoplasmic vacuolization may be seen.
Rounded cells with abundant eosinophilic cytoplasm. Can be associated with sclerotic stroma.
Most commonly (2/3’s) central lung lesions but also may be apical. Cavitation is common. The lesional cells will vary depending on the degree of differentiation. Well differentiated keratinizing lesions show cells with cytoplasmic orangeophilia and pyknotic nuclei. The cells can be rounded / polygonal to elongated / “tadpole” shaped. More poorly differentiated cases show less keratinization and are characterized more by large nuclei with a coarse chromatin texture.
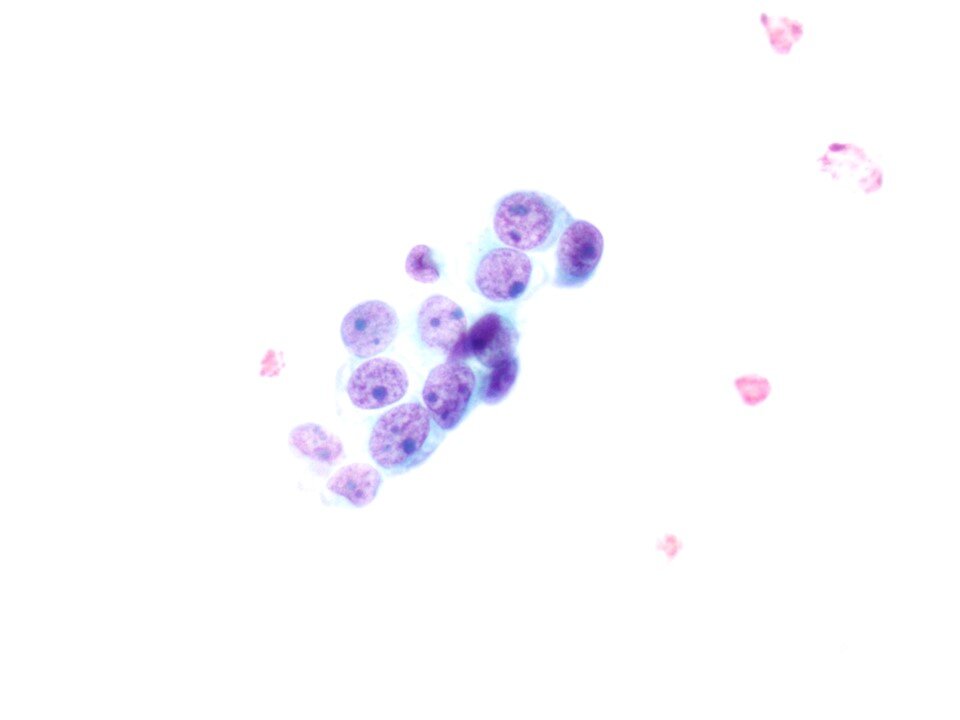
Most occur in the lung periphery. Different histologic patterns are possible, including acinar, papillary, micropapillary, and solid. Some cytomorphologic features of adenocarcinomas include cells with finely textured chromatin with large nucleoli and foamy / delicate cytoplasm +/- mucin vacuoles. The lesional cells can be identified in crowded clusters or in “drunken” honeycomb arrangements such as in this case.
Note the abundant mucin with scattered relatively bland-appearing lesional cells. These may be challenging if scant given the lack of significant cytologic atypia.
Note the mucinous cytoplasm.
Note the mucin vacuoles seen on this Pap stained smear.
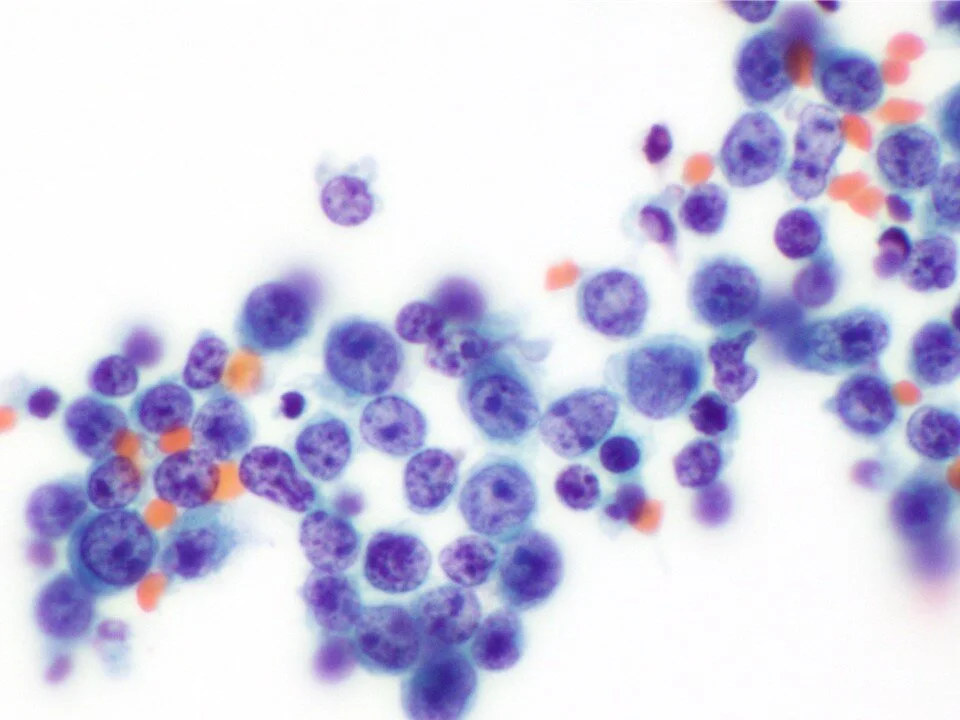
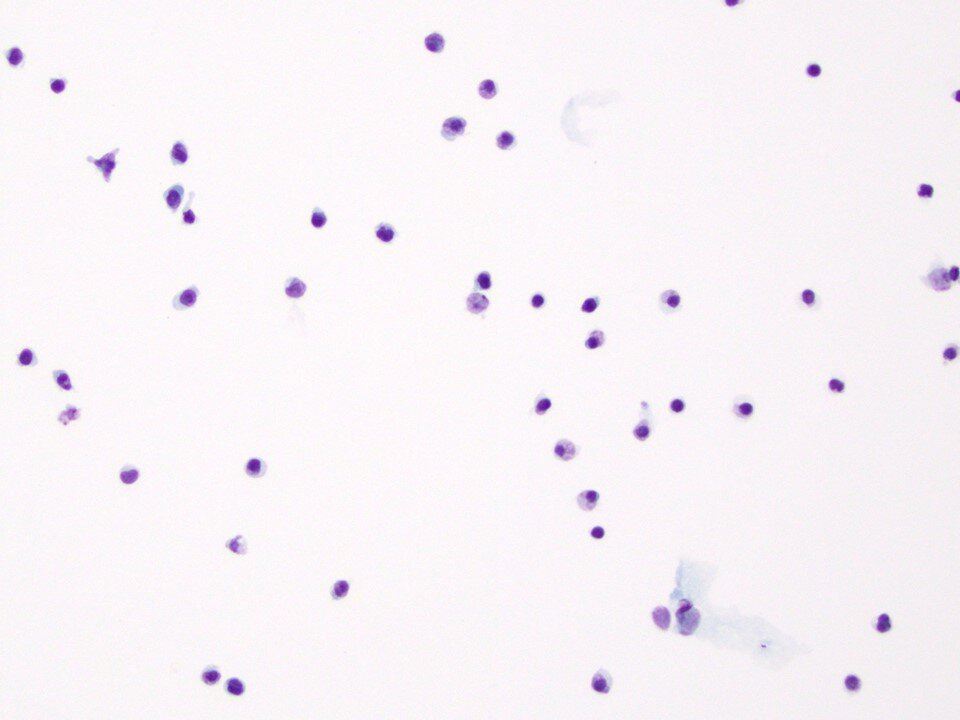
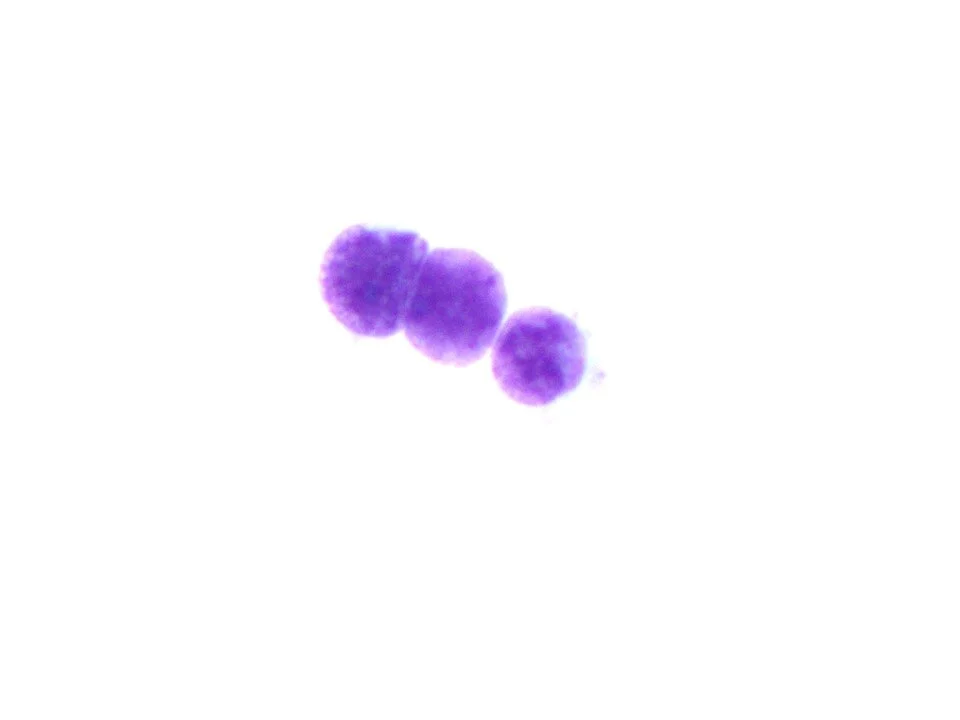
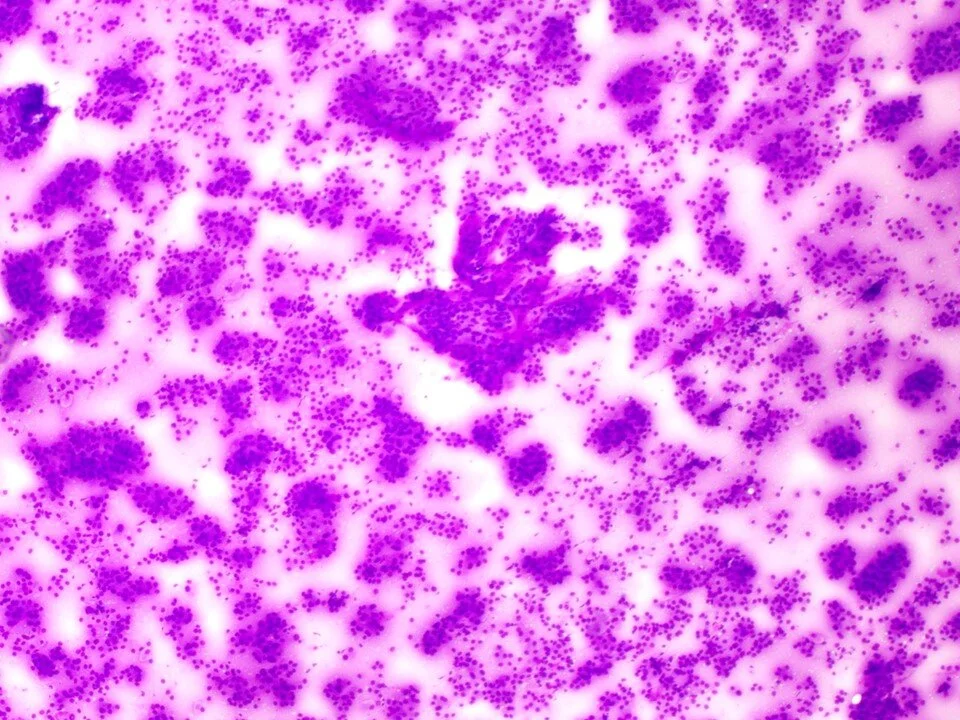
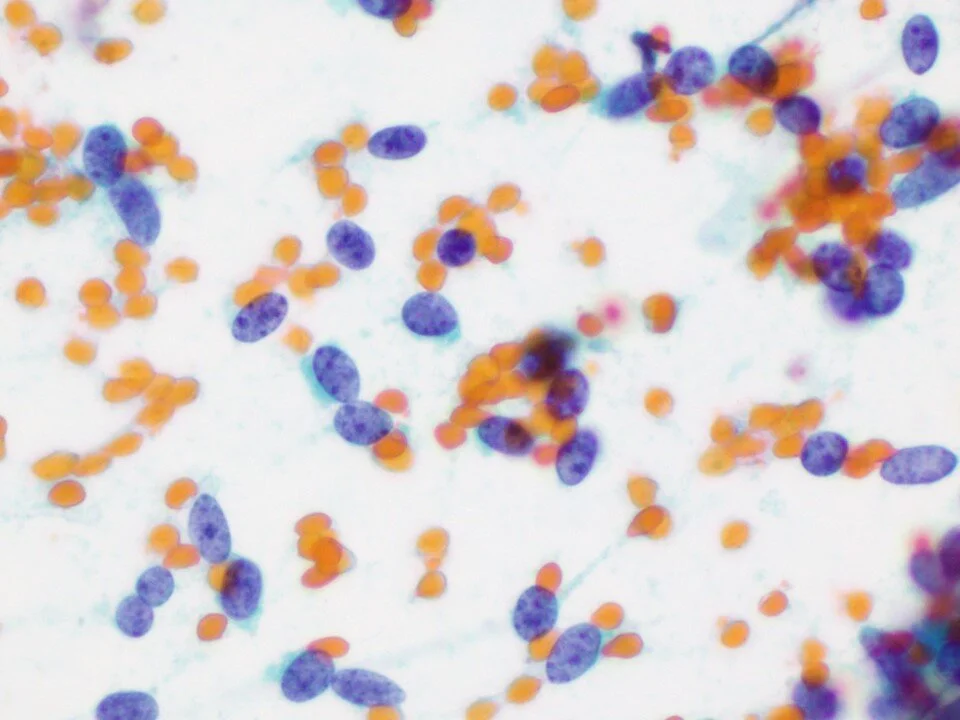
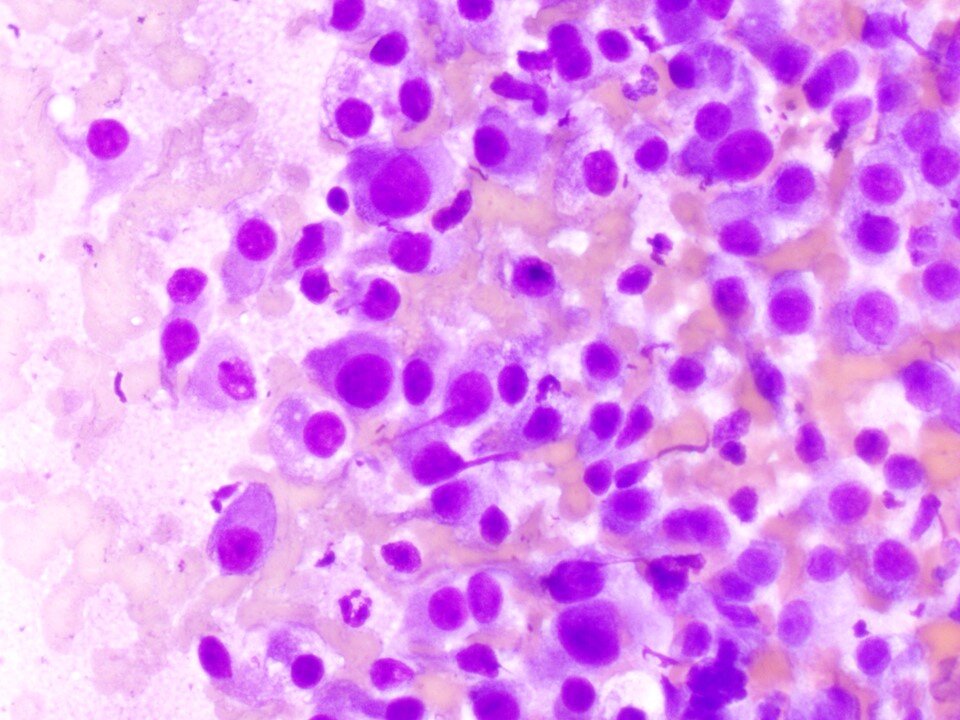
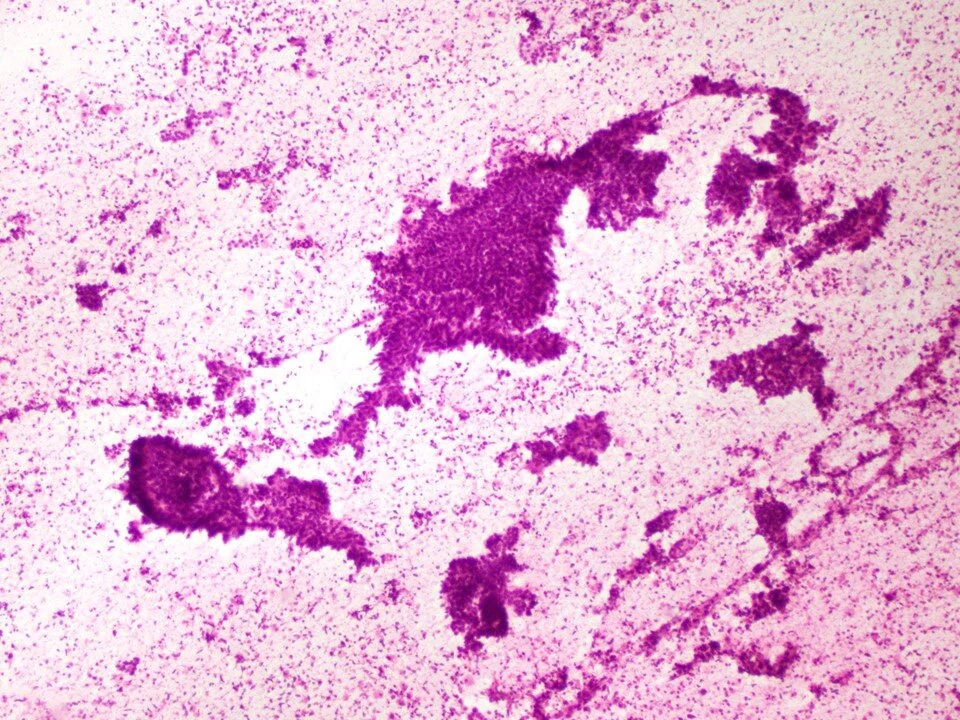
A low-grade neuroendocrine tumor with low metastatic potential. Cytologic preparations demonstrate a uniform population of cells that are arranged in a single / dispersed pattern +/- scattered clusters.
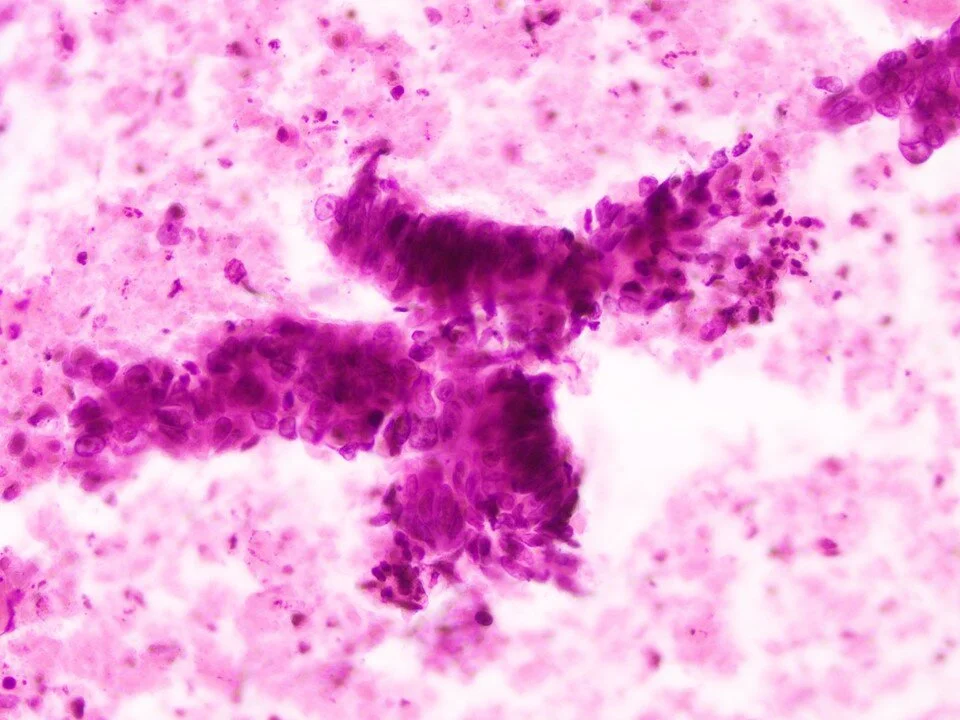
Higher magnification shows the tumor cells are round to elongated and have a finely speckled “salt and pepper” chromatin pattern.
Rosettes are seen in some cases.
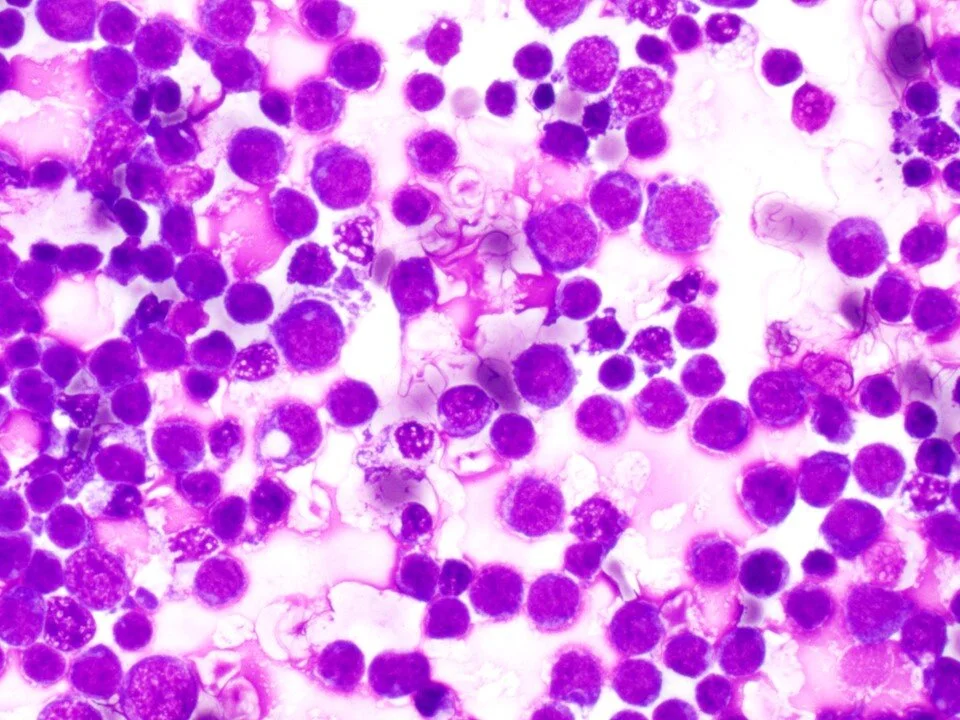
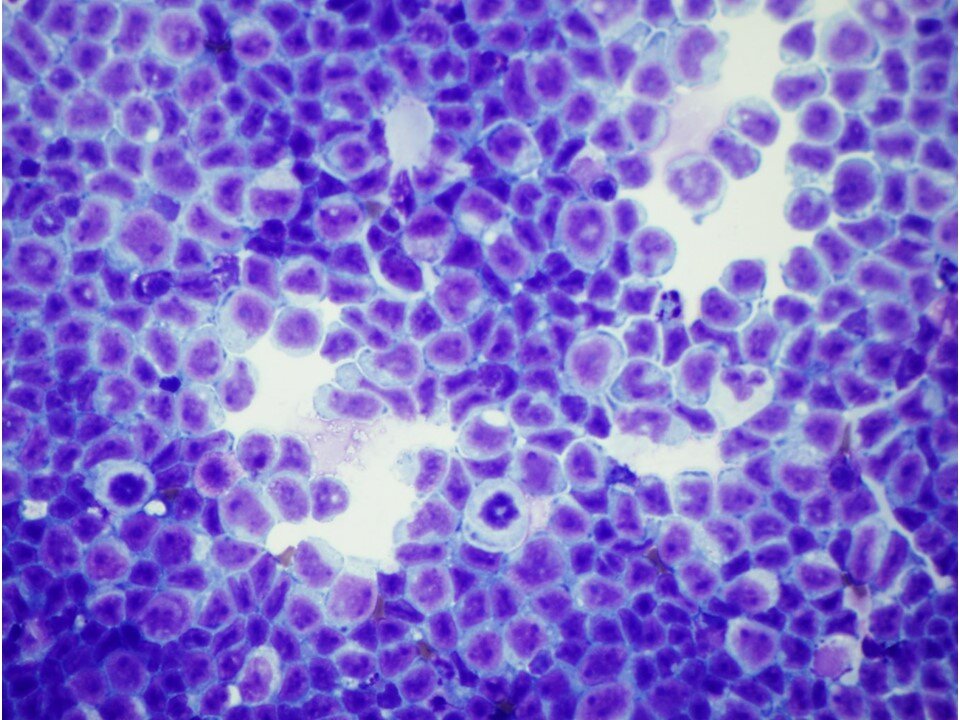
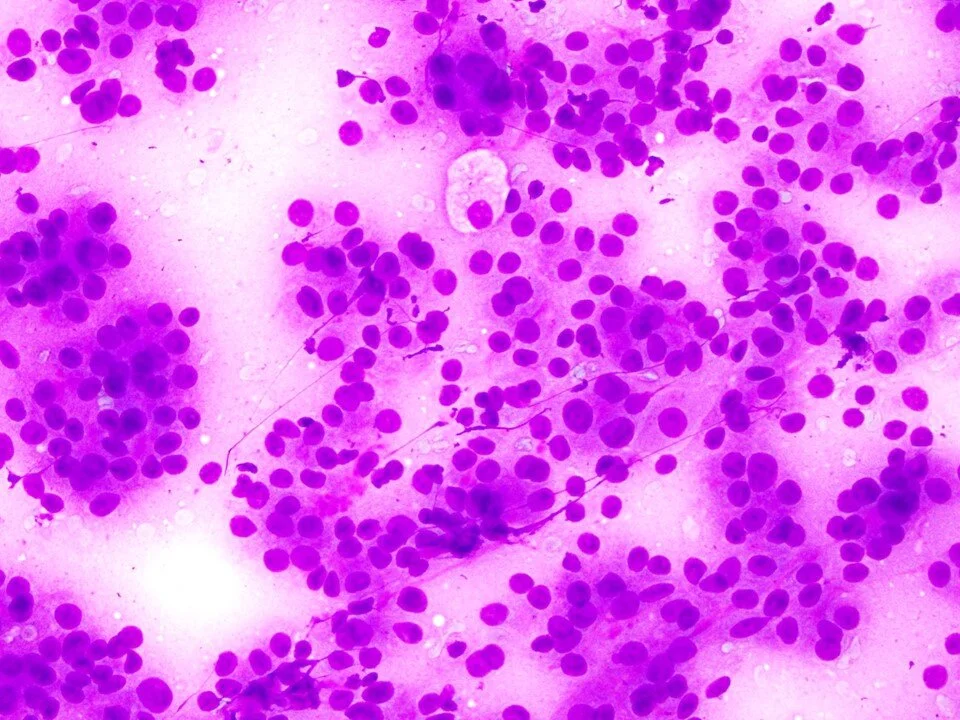
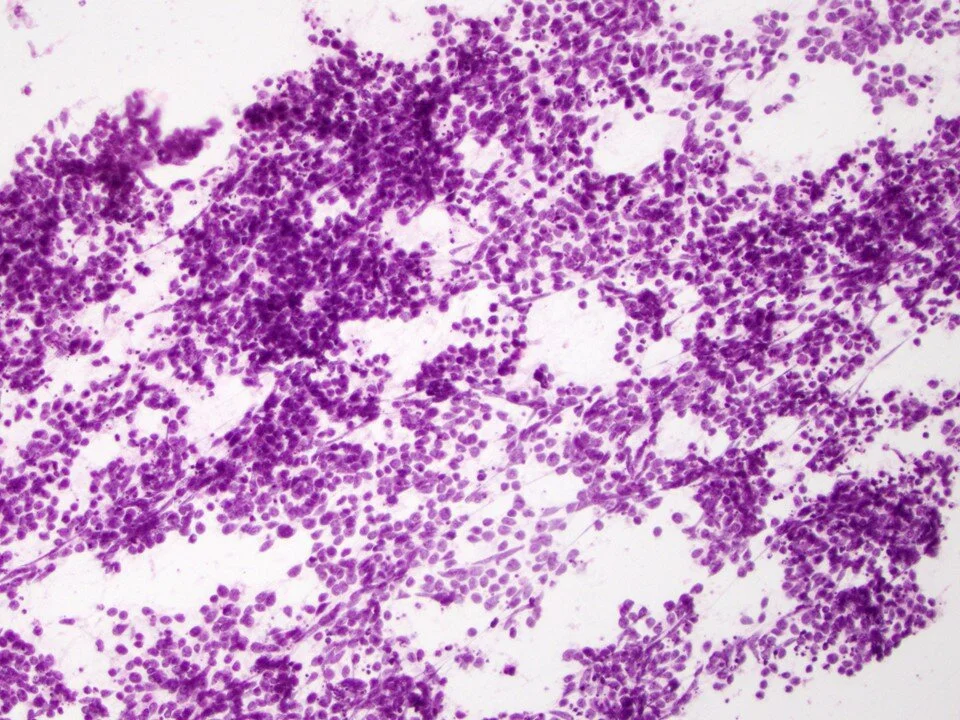
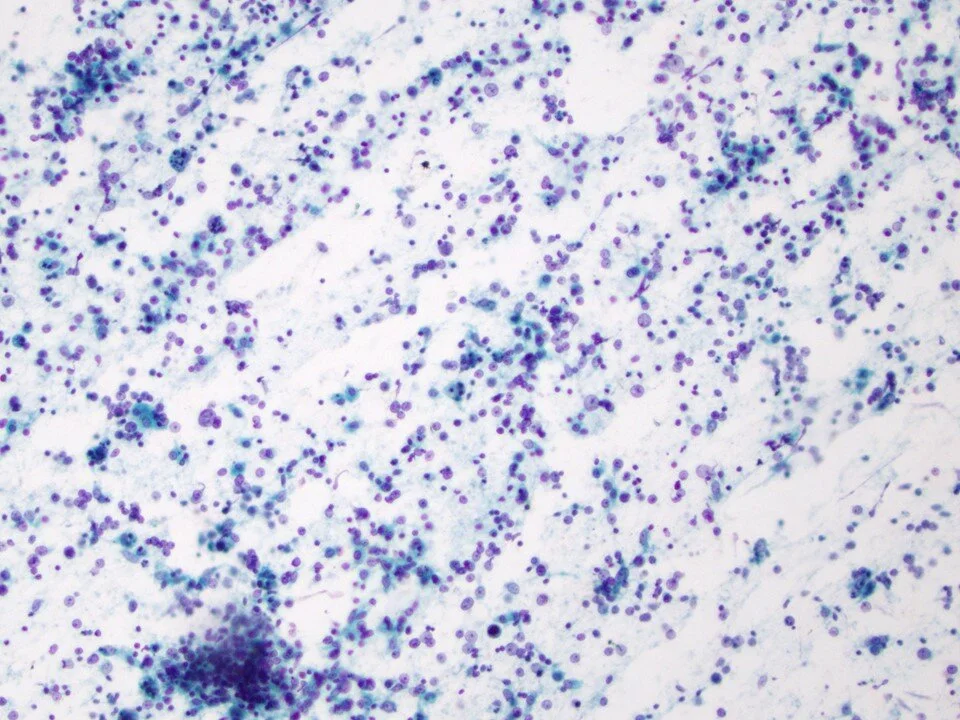
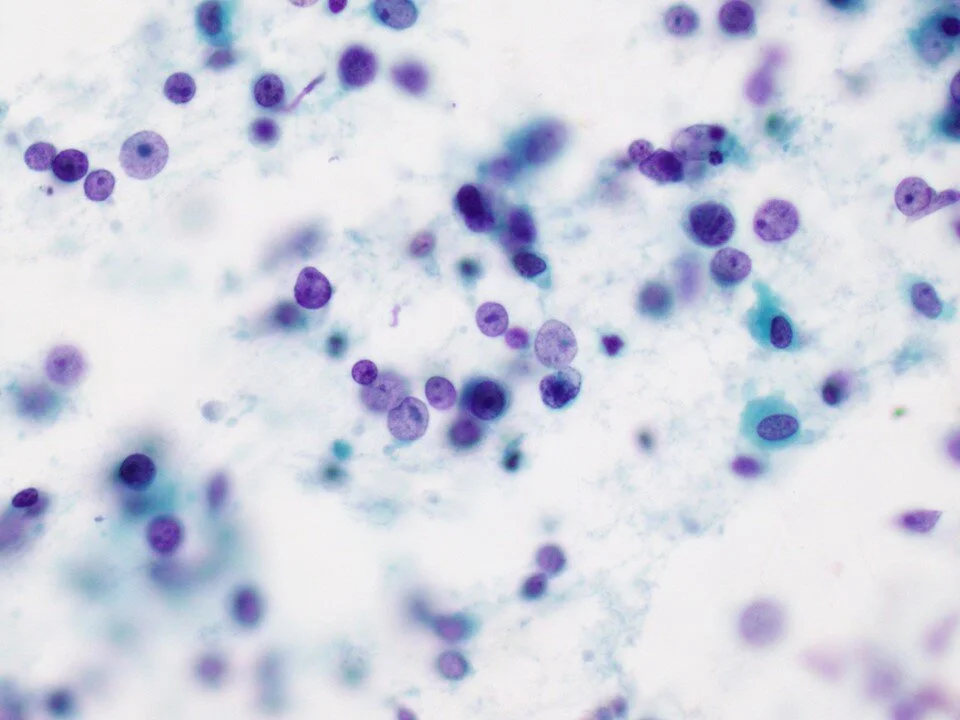
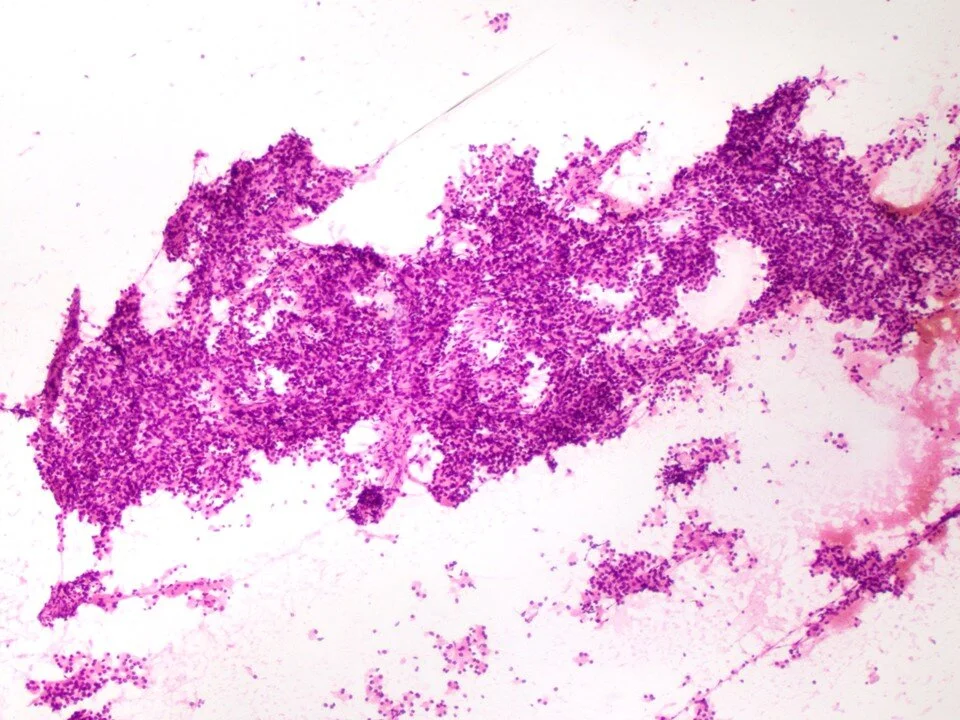
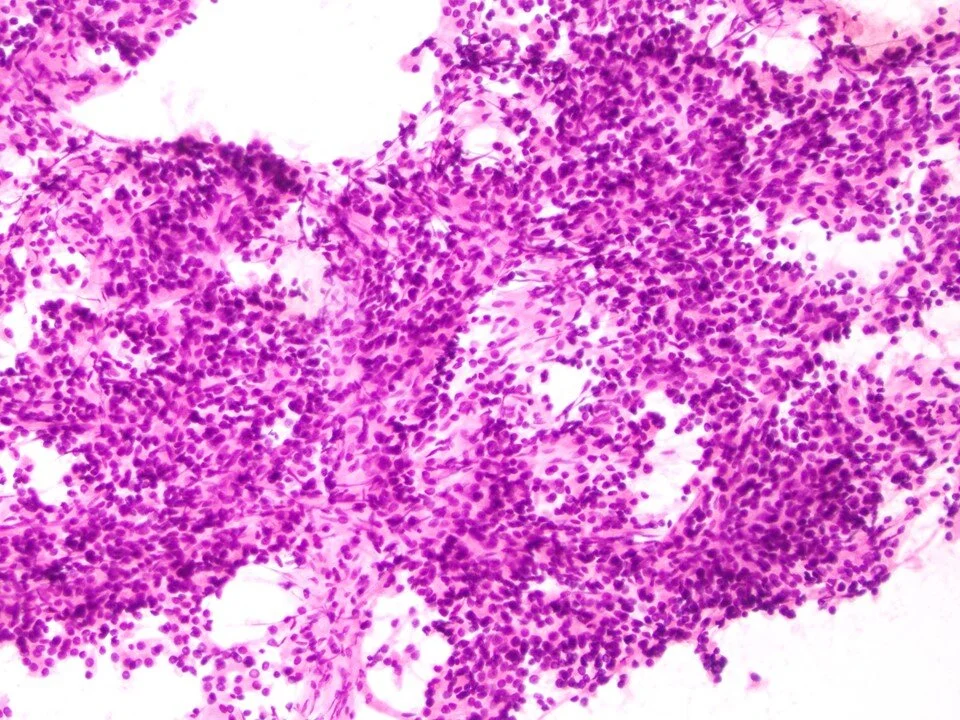
The lesional cells are found in a dispersed cell pattern. These tumors are notable for high mitotic rates, marked necrosis / apoptotic debris, and nuclear crush artifact.
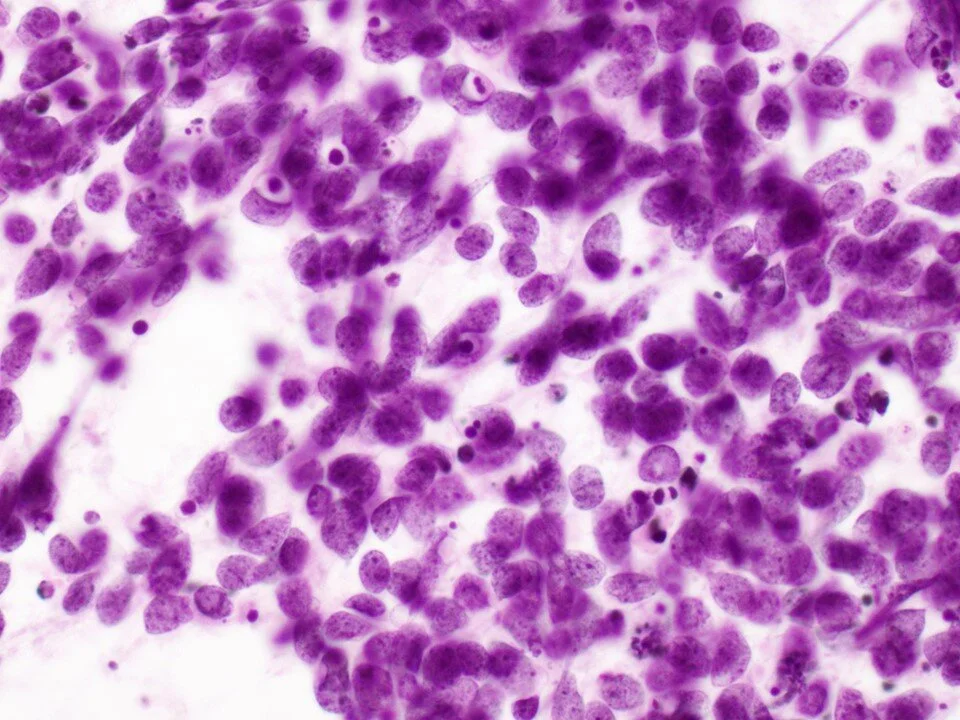
Higher magnification highlights the prominent apoptotic debris. The lesional cells have finely granular chromatin and nucleoli are inconspicuous.
Lymphomas are usually secondary to the lung, but can be primary tumors as well. Lymphomas also have a dispersed cell pattern.
Common lymphomas of the lung include extranodal marginal zone B-cell lymphoma of the mucosa-associated lymphoid tissue (MALT-lymphoma) followed by DLBCLs.
This involved the chest wall / peripheral lung.
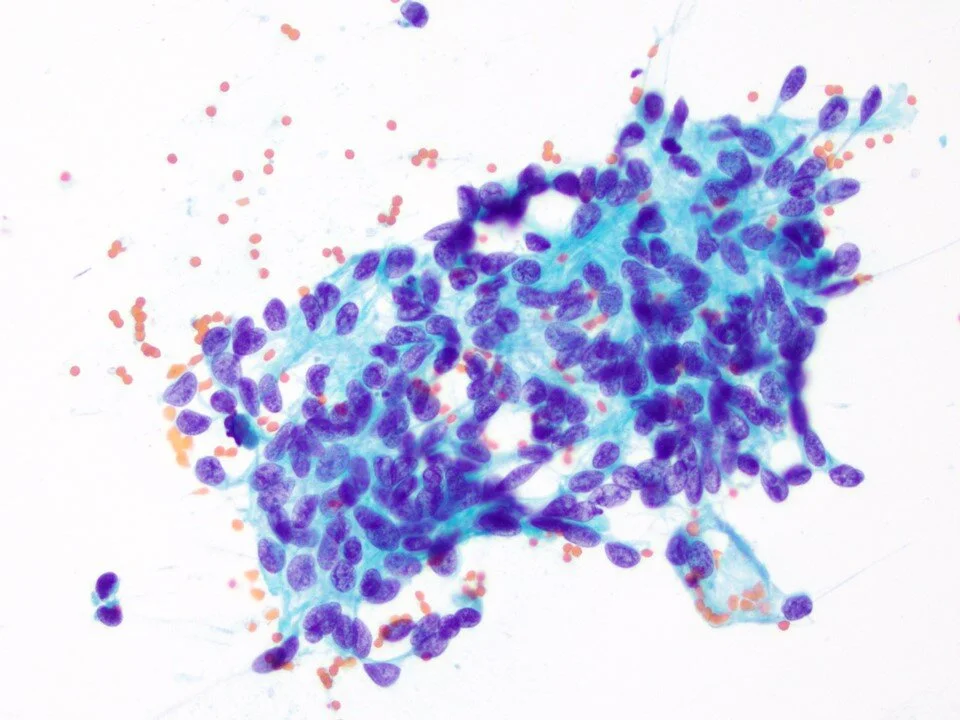
Can demonstrate a variety of patterns. This case is from an epithelioid mesothelioma.
Melanomas can take on a variety of appearances. In this case, the tumor cells were more spindled in shape.
Relatively distinctive appearance with tall columnar (picket-fence) cells, dark / hyperchromatic nuclei, and “dirty” necrosis.
Higher magnification to highlight the elongated epithelial cells and the background necrotic debris.
These are vascular tumors.
Higher magnification to highlight the vascularity
The cells are large with abundant clear to granular cytoplasm.
The tumor cells are polygonal in shape with prominent nucleoli.